Being raised under strict religious doctrine can have knock-on effects that impact all parts of life, particularly parenting, says Dr Cathy Kezelman, president of Blue Knot Foundation, an organisation that provides information and support to those suffering complex trauma. “When you’ve been raised within a controlled environment with very little freedom to make your own choices or realise that you can make choices,” she says, “it’s very difficult to develop the strong core sense of self necessary to provide your children with a secure base from which they can explore the world.”
According to Kezelman, healing begins by making sense of what has happened, how it affected you, learning self-compassion and re-evaluating your upbringing through parenting your own children. “Ways to achieve this can include counselling, self-care, meditation, yoga and art therapy. All can help to soothe the nervous system, build a sense of safety and trust and, as a parent, gradually enable your children to develop a sense of security and autonomy.”
Here, three women who have left their religion share their experiences.
“Parenting has been a healing experience” Laura McConnell Conti, 43, was a fifth-generation member of a strict fundamentalist Christian sect. Because she suffers from complex post-traumatic stress disorder, the responsibility of parenting falls on her child’s father.
“From age 12, I helped to raise my siblings. I was the eldest girl and that was what was expected of me because of our religious community’s gendered beliefs. Daily, I had to prepare their clothes, get them ready for school, help them with their homework. On the weekends I had to ensure they attended church events wearing the right dresses and having their hair in the right style. Overall, I had to keep their behaviour in line with our religious beliefs and this left me exhausted.
Wanting something different for my life, I left the church at 19. Once I got an education and a well-paying job, I was able to afford therapy. Subsequently, I spent my late 20s and 30s recovering from complex trauma – a consequence of having to worry about and care for others when I was a child myself.
At first, I didn’t want to have children. I didn’t feel I was maternal like other women seem to be, or that I had the capacity to raise a child without it impacting my health.
Eventually, I met with someone who understood that the only way I could have a child was if he was the primary carer, and I had a son in my late 30s.
I didn’t think my life would change very much, but the reality is that parenting has been a healing experience for my own childhood trauma – although that was not the intention or the expectation.
My parenting style is hands-off. I don’t have the capacity to worry or organise for my son. Difficult things, like going to the doctor or getting vaccinations, I leave to his father. I get to do more of the fun stuff – clothes shopping, hanging out and playing.
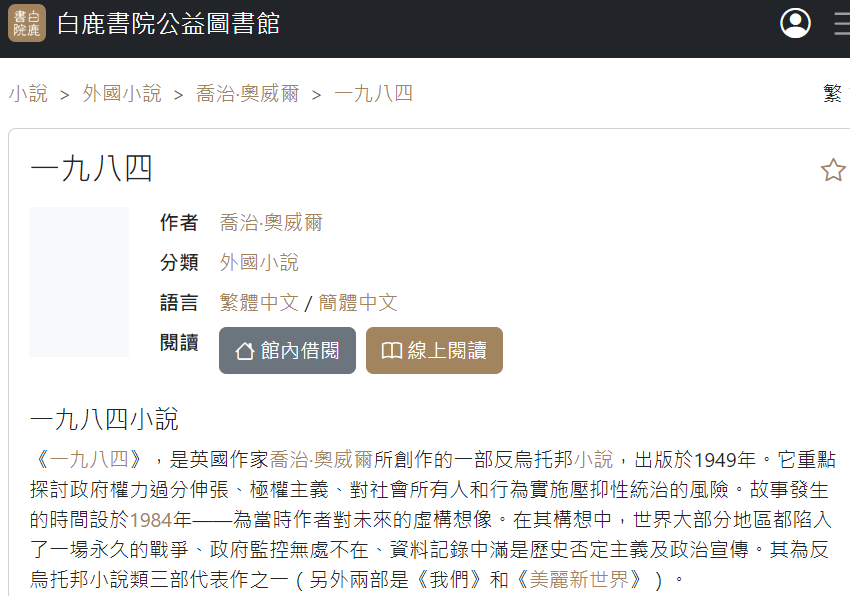
When you leave a high-control group, you don’t have a template from which to mirror good parenting. You’re relearning to do things in a very different way and, as a result, I find parenting to be a lonely experience.
And due to the abuses I experienced, I’m hyper-vigilant. This means my son hears and learns about personal safety and consent at a much younger age than most. In turn, during periods when I’m not feeling well, he understands that I can’t be completely present in his life.
I aim to raise a well-rounded human being, who can identify safe people, has the ability to be confident in life and is surrounded by good friends, so he won’t need to fill his voids from such groups.”
“The backlash from the parish was shocking” Mel Welch, 41, was born and raised under strict religious doctrine. When she left the church, she was overprotective of her children. She has since learnt that instilling self-trust is the best way to empower them.
“There were lots of rules and heavy control under the religious group I was raised in. The biggest fear instilled in me was of going to hell. It was deeply ingrained that if I upset anyone or did anything wrong, that would upset God and I would be banished to hell automatically. So I made sure not to upset the pastors or my parents.
I married a pastor’s son when I was 18 and he was 20. Marriage was the only way that being alone together would be allowed by the pastors.
Sadly, my first-born child died at birth. The backlash from the members of the parish was shocking: some said my baby’s death was because we didn’t pray enough. We were consequently given six weeks to get over our grief.
I went on to have four more children and by the time I turned 30, I could no longer keep up with the pressure I was putting on myself to attend weekly church gatherings and Sunday service. Feeling that no matter what I did I would never be enough, one Sunday afternoon in 2012 I sat opposite my husband and said, ‘I’m no longer attending church.’ My body felt nauseous from the anxiety of even hearing me say that and my husband turned white. That goes to show just how much power they had over our lives.
Consequently, I was shunned by the community. Gradually, my husband came to his own realisation and conclusion about the church and followed me six months later.
During this time, I continued to read the Bible on my own. The more I did, the more I started to listen to and trust my intuition about what the teachings meant. This is a new God, I realised. I slowly understood that I wasn’t going to die because I’d left the church. It was all a lie, so I started to wonder what else wasn’t true.
There was definitely a long transition period around figuring out how to raise my kids, because I was relearning so much and essentially becoming an adult myself. Until I was able to discern the lies from the truths, I became overprotective of them, a form of helicopter parenting, especially around any sort of religious ideas or strict ideals.
Over time, I realised that self-trust is necessary to thrive. I’ve taught my children to create a personal relationship with God through reading the Bible on their own, a relationship that’s based on self-awareness and confidence in their own instincts.”
“Marrying outside the church was frowned upon” Susannah Birch, 37, was raised in a church that discouraged her from engaging in “worldly” activities. She is teaching her children how to be independent thinkers.
“One of the main teachings I was raised on is that Christians shouldn’t be ‘worldly’. This meant I wasn’t allowed to read mainstream books – by the time I was 12, I had actually read the Bible twice – watch popular movies or wear ostentatious jewellery or make-up. Sex before marriage was considered a sin. Further, being friends with or marrying anyone from outside the church group was severely frowned upon because they were considered to be ‘evil’.
My parents divorced when I was 13, by which time my family had distanced itself from the church. To my surprise, my father, who maintained more balanced religious beliefs, allowed me to do things considered worldly. I quickly discovered the Spice Girls and Buffy the Vampire Slayer, and that began to change my whole world view. I also read different book genres and that made me question everything I had been taught growing up.
Subsequently, at age 20, I married a non-Christian. And when I had my two children, I intentionally introduced them early on to a wide range of fiction, music and movies so they could have a holistic view of the world.
Prior to becoming a parent, I thought I was over my indoctrination. Yet whenever my children did things the church would consider wrong or ‘sinful’, I was back in that world. I had to take conscious steps to prevent myself from imposing narrow ideas on my children. Today, whenever my children do something wrong, I try to explain to them why it’s wrong, as opposed to the punishments I received growing up, which I was never allowed to question.
My children attend a Catholic school, which I chose due to the quality of education it offers. It doesn’t bother me that they may be exposed to religious teachings, because at home we read and talk about multiple religions and philosophies, including paganism and Buddhism.
I’ve done my best to teach them to see different points of view and choose what they want to follow, after applying critical thinking. If they feel that something is true simply from emotions or peer pressure, I try to encourage them to question why and to think for themselves, not to be swayed by others’ opinions. I also want them to question the world around them and not to sit in self-criticism, as the church I grew up in taught me to do.”
It’s so easy to be judgy about people who get caught up in a cult, right? Even if you don’t want to be. I mean, it wouldn’t happen to us. We’d see right through all that weird stuff – like the specific language that means nothing to outsiders, knowing that only believers are on the right path, the rules which make no sense, and the charismatic leader who is clearly a bit off.
That’s what I thought when I started digging around, researching my latest novel that looks behind the walls of The Sanctuary, an imagined closed religious community dedicated to clean, organic living and environmentalism.
While there may be no single definition of a cult, they share a few potent ingredients, such as general isolation from the rest of society, an unquestioning adherence to a set of beliefs, a strict authoritarian hierarchy of power and a rock-hard sense of being among the chosen ones.Hmmm. I recognised quite a few of those ingredients. I hadn’t joined a cult. But maybe I’d been born into one.I grew up in a large Catholic family on an isolated farm outside Melbourne. I went to a Catholic school, we went to Mass on Sunday, we socialised with other Catholics. We basically didn’t mix with anybody else. We did know one or two non-Catholics and they were nice but they weren’t going to heaven. Not like us.We held a comprehensive set of beliefs that, without a normalising lens, are hard to get your head around. Such as Mary’s virgin birth, eating Christ’s body and drinking his blood, going to hell if you missed Mass on Sunday. We even had a shared language that defined us, such as transubstantiation (bread and wine in the Eucharist becomes Christ’s real body and blood) and the Blessed Trinity (three Gods in one, but really it’s just one God).
We held a comprehensive set of beliefs that, without a normalising lens, are hard to get your head around. Such as Mary’s virgin birth.
Then there were the rules about when you ate and what you ate, such as no eating before Mass, and no meat on Fridays, which I loved because we got to have fish and chips once a week – religiously. You had to regularly confess your sins, which led to considerable pre-reconciliation whispering as us kids figured out which sin we could make up this week.
And most damagingly, there was the unquestioned power of the god-like parish priest. And we all know now what that resulted in. In fact, the 2017 Royal Commission into Institutional Responses to Child Sexual Abuse inquiry identified my parish and the local boy’s secondary college as one of the active centres of paedophilia.
I didn’t question any of these rules and beliefs.
The contest of ideas I discovered at university knocked our brand of Catholicism out of me. Yet, still, years later when I had my own family, the kids eventually did some of the sacraments so they wouldn’t feel too out of place at family church events.
When my youngest child was preparing for their First Reconciliation, we dutifully read the children’s Bible stories from the Old Testament every night as requested. Now this child, who had previously declared that they wanted to be an “evil overlord” when they grew up said to me one night, “Oh mama, I’m getting a lot of good ideas about how to be an evil overlord from God.”
I laughed out loud. I hadn’t seen it before. I had completely normalised that God could legitimately require Abraham to prove his undying devotion by killing his son. Or that it was perfectly acceptable that God would test Job’s excellent piety by taking away his possessions, his family and then his health. Yeah, now that I think about it, my child was spot on: you could say that the God of the Old Testament did abuse his power as leader.
Obviously, it was a unique set of conditions that meant I experienced cult-like conditions as a child. Very few people can now live in that kind of isolation. We have the internet, which beams in all sorts of ideas all the time. As well, the modern Catholic Church has shared leadership between priests and parishioners, so authority no longer rests in a single godlike being.
There are thousands of cults across the world, from self-help cults, to political and religious cults. Many of them don’t look anything like the doomsday cult, Heaven’s Gate, which ended in mass suicide, as members tried to catch a passing comet in 1997. Or Australia’s own Ideal Human Environment, which began in the ’80s as an experiment in happiness, harmony and ideal living. In 2019, leader James Salerno was imprisoned for unlawful sexual intercourse with a child, and the truth about the abuse behind those closed doors was exposed. The IHE had been operating for 30 years.
None of us joins a cult – we join a movement to make ourselves and the world a better place. But my experience taught me that it’s a fine line between intentional community and cult. That line is defined by how power is exercised.
So, whether you’re seeking your own happiness, or a new way of making the world a better place, like that great meditation group you just joined or that conspiracy idea that is sweeping around you, take care. Watch what happens when you ask questions. If they close you down, or make you feel guilty for asking in the first place, I’m guessing it is a good idea to keep asking those questions.
As a neurosurgeon and a research scientist, dreams hold a particular fascination for me. Having spent my life immersed in the brain, I am not only infatuated with its infinite complexity but also captivated to the point of obsession by what remains one of its greatest and most mysterious features: dreaming. The source of dreams is the same as all mental activity — waves of electricity moving across the brain every moment we’re alive.
Dreams are a product of normal brain function, and an extraordinary transformation that occurs in the brain each night when we sleep, following the circadian rhythms — the day-night cycles — that biologically govern life. Each night, our brains and bodies follow a repeating 90-minute cycle of light sleep followed by deep sleep, where the brainwaves are slow and rhythmic. The eyes start rolling under their lids and most of the muscles in the body become paralysed.
When the eyes are fluttering under the eyelids, this is known as rapid eye movement or REM sleep. REM sleep and dreaming are often described as synonymous, but this is inaccurate. We can dream in all stages of sleep. But REM sleep is when the most intense and bizarre dreams occur. Dreams change as the night progresses.
Early-night dreams tend to include more elements from our waking life. Dreams at the end of the night are more likely to be emotional and incorporate older autobiographical memories, and it’s these dreams, which we have just before we wake up, that we’re most likely to remember. The tenor of our dreams shifts, too. Dreams are more negative at the beginning of the night and become more positive as the night goes on.
Dreams affect us deeply because we experience them as real. The joy we feel in dreams is physiologically no different from the joy felt when we are awake; neither is the terror, frustration, sexual excitement, anger and fear. Run in our dreams and the motor cortex is activated — the same part of your brain that you’d use if you were actually running. Feel a lover’s touch in your dream, and the sensory cortex is stimulated, just as it would be in your waking hours.
If we’re sleep deprived, the first thing we catch up on is dreaming. If we’ve had enough sleep but are dream deprived, we will immediately start dreaming as soon as we fall asleep. These days, there is much focus on needing sleep to be healthy, but it may be that it’s not the sleep we really need, but the dreams.
Erotic dreams are part of human nature. You couldn’t stop them even if you wanted to. Menopause does not extinguish them, nor does chemical castration. It doesn’t matter whether you are sexually active, celibate, married or single. Erotic dreams are universal. In surveys, sexual dreams were reported by 90 per cent of Brits, 87 per cent of Germans, 77 per cent of Canadians, 70 per cent of Chinese, 68 per cent of Japanese, and 66 per cent of Americans.
An estimated one in 12 of all dreams contains sexual imagery, the commonest being, in order: kissing, intercourse, sensual embrace oral sex and masturbation. The dreams can leave us flushed with pleasure or filled with jealousy. They are often unsettling, too. What does it mean to have a sexual dream about an ex?
What if your partner has one about someone else? Do they reveal anything about our desires? single men have a higher frequency of erotic dreams compared to men in stable partnerships. On the other hand, women report more sexual dreams when they miss their partners or are at the height of a love affair. Men report no similar surge in erotic dreams in those scenarios. But there’s one way in which the dreaming life of men and women align — almost all of us cheat in our dreams.
What should we make of this? As creators of our dreams, we select the cast of our nocturnal dramas, the stage and the action. The dreams we conjure are our own sensual productions. Wouldn’t a dream where we cheat on a partner be a sign that we are looking to be unfaithful, or are at least open to it? Surely an erotic dream is our libido unfiltered and unleashed. If not, then what could it possibly be? All dreams are the product of the Imagination Network in our brains, unbound by the rules and logic of our waking life.
When we’re dreaming, the imagination is unfettered, free to find loose associations and connections in our memories. It can lead us to think about the people in our lives in surprising, disturbing and even erotic ways. Because the logical Executive Network in our brains is shut down during dreaming, we can’t stop these erotic flights of fancy before they take off.
They are also free from judgment — even our own. In erotic dreams we are liberated to imagine sexual encounters that would be taboo or inconceivable in our waking lives. They will probably not involve our current partner. Instead, we have more of an inclination towards novel sexual interactions. So, what do erotic dreams really mean? Researchers have conducted surveys on sexual activity, asking how happy people are in their romantic relationships, whether they have jealous personalities and how these characteristics impact on their dreams.
The scientists tried to provoke erotic dreams by asking participants to watch porn. What they found was surprising. Erotic dreams are not tied to how much sex you are having in your waking life, nor to whether you masturbate. They are not even connected to how much porn you consume. The best predictor of erotic dreaming seems to be how much of our waking life we spend daydreaming about erotic fantasies.
This makes us more open to erotic dreams at night. However, there’s one key difference between daytime fantasies and erotic dreams. When we fantasise during the day, our thoughts are reined in by the rational part of our brain, the Executive Network , which constrains sexual desires. This moderating influence is gone when we dream, allowing our erotic dreams to be wildly creative and exploratory.
From this I conclude that erotic dreams are more like thought experiments than a sign of the type of latent desires that Freud wrote about. We can switch genders or become bisexual, even if it never crosses our minds during the day. Erotic dreams are undeniably deeply pleasurable. In a survey of university students in China, they agreed overwhelmingly with the following statements: ‘I hope to immerse myself in a sexual dream and never wake up’, ‘I feel lucky to have sexual dreams’, and ‘I am sad after waking up from a sexual dream because I find it was just a dream.’
How can it be that imagined sex carries such emotional, libidinal weight? These are, after all, solitary, imagined events outside of our conscious control. It seems implausible that they could mean so much to us, but they do. The answer is that erotic dreams have this kind of power because the brain is our most powerful sex organ. Erotic dreams do more than just reflect or release our emotions, imagination and libido.
They can deliver the same intense pleasure as actual sex. They might even be better than the real thing. In erotic dreams, the brain is not receiving any signals of touching or of being touched. Erotic dreams occur in the brain alone. Even so, more than two-thirds of men and more than a third of women say they’ve experienced orgasms simply as the result of a dream. Consider what is happening in the brain during the physical act of sex.
Sexual activity draws upon every bit of our central nervous system, which sends signals to the brain during sex. The crucial thing is that the brain interprets them. You can be touched in the same place, with the same pressure, in the same fashion, and your brain can view it as something insignificant. Or see it as a frisson or a caress. In which case, it doesn’t matter where you’re touched. The brain alone is what determines sexual significance, causes us to feel attraction (or not), to become aroused (or not), our breathing to quicken (or not) and our heart to race (or not). In erotic dreams, however, the body is silent.
During our most vivid dreams, muscles needed for coordinated movement are essentially paralysed below the neck. The brain is not reacting to signals from the body, but is instead acting out its own imagination. As erotic dreams show us, the brain doesn’t need the rest of the body at all. The mind is its own erogenous zone, and dreams can pursue the pleasures of the flesh without any flesh other than the brain itself.
If this all sounds impossible, think about other aspects of how we perceive and respond to the world. Consider sight, for example. The lens and cornea work together to focus light on the retina at the back of the eye, but it is the brain that processes what is seen into a single, clear view of the world. Without the brain, we do not see. Erotic dreams are the same. With no sensory inputs at all, the brain creates and perceives full-bodied pleasure.
Sex and other erotic pleasures we experience in our dreams are not felt any differently because, as far as the brain is concerned, there is no difference. The brain does not experience real orgasms or fake ones; to the brain, they are all real. And since, during dreams, our unrestrained emotional system can exceed levels we reach in waking life, it’s reasonable to conclude that a dream orgasm can take us to heights that waking sex cannot. What, then, do erotic dreams reveal about our relationships?
The science suggests that dreams of infidelity are unlikely to be a signal that we want to be unfaithful. They are far more likely to be the brain’s Imagination Network in action. Cheating on a partner in a dream may simply be a sign of curiosity and normal sexual arousal, rather than a desire to stray from the relationship. Nor are dreams where we explore a different sexual orientation a sign of a repressed desire.
This, too, appears to be more curiosity, libido and imagination at play. Even so, erotic dreams have plenty to tell us about both the health of our current romantic relationships and how well we have got over former partners, but perhaps not in the way we may expect. Sexual dreams can elicit strong feelings of desire, jealousy, love, sadness or joy powerful enough to affect how we feel about our partner the next day.
Just like the sensations in the dream, the brain perceives the emotions as real. Researchers have found conflict with a partner in a dream tends to result in conflict the following day. In unhealthy relationships, infidelity dreams are associated with decreased feelings of love and intimacy in the days that follow. In healthy relationships, infidelity dreams don’t have much of an effect at all. How we feel about a partner during our waking hours can also affect our dreams.
Feelings of jealousy during the day can produce dreams of infidelity, which in turn affect a dreamer’s behaviour towards their partner. In these cases, dreams and reality appear to feed on each other in a negative loop. It’s likely that negative emotions in an erotic dream about a partner could serve as an important signal of how you feel about that person. But the emotions associated with erotic dreams are far more important than the dream narrative itself.
If you or your partner have a dream of being unfaithful, this is not a sign of anyone’s true desires. Even though you may wake up unsettled or upset, remember that dreams are designed to make us think divergently, including about our sex lives. What really counts is not our erotic dream narrative or our partner’s, but how we react to these dreams.
Ex-pARTNERS can and do show up in dreams long after they have ceased to be a part of our lives. While dreams of current partners often involve doing something together, dreams of ex-partners are more likely to be erotic. You may be tempted to conclude that this means we’re longing for an ex. But based on a number of studies, the opposite is usually true.
These dreams appear to be helping us to get over our former partners. They may simply be a way of processing the emotions of a break-up. There may, though, be a more fundamental purpose to erotic dreams — as a way our brains have evolved to protect humanity and prepare it for procreation.
My belief is that erotic dreams are a cognitive platform on which sexual fluidity and ingenuity are created; ‘wildcards’ that could help our species to survive by giving us flexible desires so that we have the means to reproduce even in the most extreme circumstances. If, say, half our tribe was wiped out by disease, erotic dreams like these could have readied our ancestors for new engagements and entanglements within our tribe.
This may also help explain why erotic dreams tend to stick close to home. The characters in our erotic dreams are rarely inventive, but the interactions often are. In this way, erotic dreams are more than our true desires — they are the embodiment of desire itself. They prime us for sexual exploration and a breadth of sexual impulses. This makes sense when we remember that the essential biological imperative of life is to survive long enough to reproduce. Our brains have developed so they are highly tuned to erotic thinking. Fantasy, erotic dreaming — and ultimately our sexuality — arose from the drive to procreate.
BECAUSE the game of hide-and-seek was still going on, it took Edmund and Lucy some time to find the others. But when at last they were all together (which happened in the long room, where the suit of armour was) Lucy burst out:
“Peter! Susan! It’s all true. Edmund has seen it too. There is a country you can get to through the wardrobe. Edmund and I both got in. We met one another in there, in the wood. Go on, Edmund; tell them all about it.”
“What’s all this about, Ed?” said Peter.
And now we come to one of the nastiest things in this story. Up to that moment Edmund had been feeling sick, and sulky, and annoyed with Lucy for being right, but he hadn’t made up his mind what to do. When Peter suddenly asked him the question he decided all at once to do the meanest and most spiteful thing he could think of. He decided to let Lucy down.
“Tell us, Ed,” said Susan.
And Edmund gave a very superior look as if he were far older than Lucy (there was really only a year’s difference) and then a little snigger and said, “Oh, yes, Lucy and I have been playing – pretending that all her story about a country in the wardrobe is true. just for fun, of course. There’s nothing there really.”
Poor Lucy gave Edmund one look and rushed out of the room.
Edmund, who was becoming a nastier person every minute, thought that he had scored a great success, and went on at once to say, “There she goes again. What’s the matter with her? That’s the worst of young kids, they always – “
“Look here,” said Peter, turning on him savagely, “shut up! You’ve been perfectly beastly to Lu ever since she started this nonsense about the wardrobe, and now you go playing games with her about it and setting her off again. I believe you did it simply out of spite.”
“But it’s all nonsense,” said Edmund, very taken aback.
“Of course it’s all nonsense,” said Peter, “that’s just the point. Lu was perfectly all right when we left home, but since we’ve been down here she seems to be either going queer in the head or else turning into a most frightful liar. But whichever it is, what good do you think you’ll do by jeering and nagging at her one day and encouraging her the next?”
“I thought – I thought,” said Edmund; but he couldn’t think of anything to say.
“You didn’t think anything at all,” said Peter; “it’s just spite. You’ve always liked being beastly to anyone smaller than yourself; we’ve seen that at school before now.”
“Do stop it,” said Susan; “it won’t make things any better having a row between you two. Let’s go and find Lucy.”
It was not surprising that when they found Lucy, a good deal later, everyone could see that she had been crying. Nothing they could say to her made any difference. She stuck to her story and said:
“I don’t care what you think, and I don’t care what you say. You can tell the Professor or you can write to Mother or you can do anything you like. I know I’ve met a Faun in there and – I wish I’d stayed there and you are all beasts, beasts.”
It was an unpleasant evening. Lucy was miserable and Edmund was beginning to feel that his plan wasn’t working as well as he had expected. The two older ones were really beginning to think that Lucy was out of her mind. They stood in the passage talking about it in whispers long after she had gone to bed.
The result was the next morning they decided that they really would go and tell the whole thing to the Professor. “He’ll write to Father if he thinks there is really something wrong with Lu,” said Peter; “it’s getting beyond us.” So they went and knocked at the study door, and the Professor said “Come in,” and got up and found chairs for them and said he was quite at their disposal. Then he sat listening to them with the tips of his fingers pressed together and never interrupting, till they had finished the whole story. After that he said nothing for quite a long time. Then he cleared his throat and said the last thing either of them expected:
“How do you know,” he asked, “that your sister’s story is not true?”
“Oh, but – ” began Susan, and then stopped. Anyone could see from the old man’s face that he was perfectly serious. Then Susan pulled herself together and said, “But Edmund said they had only been pretending.”
“That is a point,” said the Professor, “which certainly deserves consideration; very careful consideration. For instance – if you will excuse me for asking the question – does your experience lead you to regard your brother or your sister as the more reliable? I mean, which is the more truthful?”
“That’s just the funny thing about it, sir,” said Peter. “Up till now, I’d have said Lucy every time.”
“And what do you think, my dear?” said the Professor, turning to Susan.
“Well,” said Susan, “in general, I’d say the same as Peter, but this couldn’t be true – all this about the wood and the Faun.”
“That is more than I know,” said the Professor, “and a charge of lying against someone whom you have always found truthful is a very serious thing; a very serious thing indeed.”
“We were afraid it mightn’t even be lying,” said Susan; “we thought there might be something wrong with Lucy.”
“Madness, you mean?” said the Professor quite coolly. “Oh, you can make your minds easy about that. One has only to look at her and talk to her to see that she is not mad.”
“But then,” said Susan, and stopped. She had never dreamed that a grown-up would talk like the Professor and didn’t know what to think.
“Logic!” said the Professor half to himself. “Why don’t they teach logic at these schools? There are only three possibilities. Either your sister is telling lies, or she is mad, or she is telling the truth. You know she doesn’t tell lies and it is obvious that she is not mad For the moment then and unless any further evidence turns up, we must assume that she is telling the truth.”
Susan looked at him very hard and was quite sure from the expression on his face that he was no making fun of them.
“But how could it be true, sir?” said Peter.
“Why do you say that?” asked the Professor.
“Well, for one thing,” said Peter, “if it was true why doesn’t everyone find this country every time they go to the wardrobe? I mean, there was nothing there when we looked; even Lucy didn’t pretend the was.”
“What has that to do with it?” said the Professor.
“Well, sir, if things are real, they’re there all the time.”
“Are they?” said the Professor; and Peter did’nt know quite what to say.
“But there was no time,” said Susan. “Lucy had no time to have gone anywhere, even if there was such a place. She came running after us the very moment we were out of the room. It was less than minute, and she pretended to have been away for hours.”
“That is the very thing that makes her story so likely to be true,” said the Professor. “If there really a door in this house that leads to some other world (and I should warn you that this is a very strange house, and even I know very little about it) – if, I say, she had got into another world, I should not be at a surprised to find that the other world had a separate time of its own; so that however long you stay there it would never take up any of our time. On the other hand, I don’t think many girls of her age would invent that idea for themselves. If she had been pretending, she would have hidden for a reasonable time before coming out and telling her story.”
“But do you really mean, sir,” said Peter, “that there could be other worlds – all over the place, just round the corner – like that?”
“Nothing is more probable,” said the Professor, taking off his spectacles and beginning to polish them, while he muttered to himself, “I wonder what they do teach them at these schools.”
“But what are we to do?” said Susan. She felt that the conversation was beginning to get off the point.
“My dear young lady,” said the Professor, suddenly looking up with a very sharp expression at both of them, “there is one plan which no one has yet suggested and which is well worth trying.”
“What’s that?” said Susan.
“We might all try minding our own business,” said he. And that was the end of that conversation.
After this things were a good deal better for Lucy. Peter saw to it that Edmund stopped jeering at her, and neither she nor anyone else felt inclined to talk about the wardrobe at all. It had become a rather alarming subject. And so for a time it looked as if all the adventures were coming to an end; but that was not to be.
This house of the Professor’s – which even he knew so little about – was so old and famous that people from all over England used to come and ask permission to see over it. It was the sort of house that is mentioned in guide books and even in histories; and well it might be, for all manner of stories were told about it, some of them even stranger than the one I am telling you now. And when parties of sightseers arrived and asked to see the house, the Professor always gave them permission, and Mrs Macready, the housekeeper, showed them round, telling them about the pictures and the armour, and the rare books in the library. Mrs Macready was not fond of children, and did not like to be interrupted when she was telling visitors all the things she knew. She had said to Susan and Peter almost on the first morning (along with a good many other instructions), “And please remember you’re to keep out of the way whenever I’m taking a party over the house.”
“Just as if any of us would want to waste half the morning trailing round with a crowd of strange grown-ups!” said Edmund, and the other three thought the same. That was how the adventures began for the second time.
A few mornings later Peter and Edmund were looking at the suit of armour and wondering if they could take it to bits when the two girls rushed into the room and said, “Look out! Here comes the Macready and a whole gang with her.”
“Sharp’s the word,” said Peter, and all four made off through the door at the far end of the room. But when they had got out into the Green Room and beyond it, into the Library, they suddenly heard voices ahead of them, and realized that Mrs Macready must be bringing her party of sightseers up the back stairs – instead of up the front stairs as they had expected. And after that – whether it was that they lost their heads, or that Mrs Macready was trying to catch them, or that some magic in the house had come to life and was chasing them into Narnia they seemed to find themselves being followed everywhere, until at last Susan said, “Oh bother those trippers! Here – let’s get into the Wardrobe Room till they’ve passed. No one will follow us in there.” But the moment they were inside they heard the voices in the passage – and then someone fumbling at the door – and then they saw the handle turning.
“Quick!” said Peter, “there’s nowhere else,” and flung open the wardrobe. All four of them bundled inside it and sat there, panting, in the dark. Peter held the door closed but did not shut it; for, of course, he remembered, as every sensible person does, that you should never never shut yourself up in a wardrobe.
Photos by Benjamin Brink The Oregonian October 1, 2000, Part 1
At a certain age, nothing is more important than fitting in
The boy sits on the living room sofa, lost in his thoughts and stroking the family cat with his fragile hands. His younger brother and sister sit on the floor, chattering and playing cards. But Sam is overcome by an urge to be alone. He lifts the cat off his lap, ignoring a plaintive meow, and silently stands, tottering unsteadily as his thin frame rises in the afternoon light.
He threads his way toward the kitchen, where his mother bends over the sink, washing vegetables for supper. Most 14-year-old boys whirl through a room, slapping door jambs and dodging around furniture like imaginary halfbacks. But this boy, a 5-foot, 83-pound waif, has learned never to draw attention to himself. He moves like smoke.
He stops in the door frame leading to the kitchen and melts into the late-afternoon shadows.
He watches his mother, humming as she runs water over lettuce. The boy clears his throat and says he’s not hungry. His mother sighs with worry and turns, not bothering to turn off the water or to dry her hands. The boy knows she’s studying him, running her eyes over his bony arms and the way he wearily props himself against the door frame. She’s been watching him like this since he left the hospital a few months before.
“I’m full,” he says.
She bends her head toward him, about to speak. He cuts her off.
“Really, Mom. I’m full.”
“OK, Sam,” she says quietly.
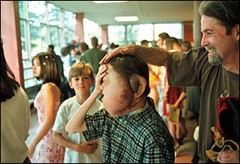
The boy slips behind his mother and steps into a pool of light.
A huge mass of flesh balloons out from the left side of his face.
His left ear, purple and misshapen, bulges from the side of his head. His chin juts forward. The main body of tissue, laced with blue veins, swells in a dome that runs from sideburn level to chin. The mass draws his left eye into a slit, warps his mouth into a small, inverted half moon. It looks as though someone has slapped three pounds of wet clay onto his face, where it clings, burying the boy inside.
Sam Lightner at a meeting of his Boy Scout troop.
But Sam, the boy behind the mask, peers out from the right eye. It is clear, perfectly formed and a deep, penetrating brown.
You find yourself instantly drawn into that eye, pulled past the deformity and into the world of a completely normal 14-year-old. It is a window into the world where Sam lives. You can imagine yourself on the other side of it. You can see yourself in that eye, the child you once were.
The third of Sam’s face surrounding his normal eye reinforces the impression. His healthy, close-cropped hair is a luxuriant brown, shaped carefully in a style any serious young man might wear. It’s trimmed neatly behind a delicate, well-formed ear. His right cheek glows with the blushing good health that the rest of his face has obscured.
The boy passes out of the kitchen, stepping into the staircase that leads to the second floor. A ragged burst of air escapes from the hole in his throat—a tracheotomy funnels air directly into his lungs, bypassing the swollen tissue that blocks the usual airways. He walks along the worn hallway and turns into his room, the one with the toy license plate on the door. It reads “Sam.”
The Northeast Portland house, wood-framed with a wide front porch and fading cream-colored paint, is like thousands of others on Portland’s gentrifying eastside. Real estate prices have soared, but the Lightners still need new carpets in every room and could use new appliances. Although she’d rather stay home with the children, Debbie Lightner works part time as a bank teller. The paycheck helps, but she really took the job for the health insurance.
From upstairs, Sam hears 12-year-old Emily and 9-year-old Nathan laughing. The kitchen, though, is silent. The boy figures his mother and father are talking about him and this night. For months Feb. 3, 2000, has been circled on the family calendar that hangs on a kitchen wall.
He grabs a small foam basketball and throws up an arcing shot that soars across the room and hits a poster tacked to the far wall.
His mother made the poster by assembling family photographs and then laminating them. In the middle is a questionnaire Sam filled out when he was 8. He had been asked to list his three wishes. He wanted $1 million and a dog. On the third line, he doodled three question marks—in those oblivious days of childhood, he couldn’t think of anything else he needed.
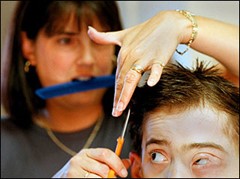
The morning routine around the family’s Northeast Portland house gets hectic when five Lightners line up for one bathroom, hunt for socks, eat breakfast and rush out the door. But Debbie Lightner still finds time for play with Sam as she challenges his decision about the shirt he’ll wear to school.
Finally, his mother calls out. His teeth are brushed, his face washed. He runs his left hand through his brown hair, parting it to the right.
He must imagine what he looks like. There’s no mirror to examine his face.
In this boy’s room, there’s never been a mirror.
“Ready for this, Sam?” asks David Lightner, a weathered jewelry designer who saves money by riding a motorcycle 25 miles to work. Sam nods his head and replies with a garbled sound, wheezing and breathless, the sound of an old man who has smoked too long and too hard.
“OK,” his father replies. “Let’s go.”
His sister and brother watch from the window as Sam and his parents walk to a Honda Accord that has 140,000 hard miles on the odometer. The boy gets in the back seat, and the Honda backs down the driveway.
Just a few blocks from home, Sam senses someone looking at him. After a lifetime of stares, he can feel the glances.
The Accord is stopped at a light, waiting to turn west onto Northeast Sandy Boulevard, when a woman walking a poodle catches sight of him. She makes no pretense of being polite, of averting her eyes. When the light changes, the woman swivels her head as if watching a train leave a station.
On school mornings, Sam rustles up his own breakfast, and his sweet tooth sometimes gets the better of him. His wholesome side might lead him to microwave a bowl of hot cereal. But he’s just as likely to top it with chocolate syrup.
Grant High School’s open house attracts more than 1,500 students and parents. Even though they’ve come early, the Lightners must search for a parking place. Sam’s father circles the streets until he finds one nearly 15 blocks from the school.
The family steps out onto the sidewalk and walks through the dark neighborhood. As Sam passes under a streetlight, a dark-green Range Rover full of teen-age boys turns onto the street. A kid wearing a baseball cap points at the boy. The car slows. The windows fill with faces, staring and pointing.
Sam walks on.
Soon, the streets fill with teen-agers on their way to Grant. Sam recognizes a girl who goes to his school, Gregory Heights Middle School. Sam has a secret crush on her. She has brown hair, wavy, and a smile that makes his hands sweat and his heart race when he sees her in class.
“Hi, Sam,” she says.
He nods.
“Hi,” he says.
The boy’s parents fall behind, allowing their son and the girl to walk side by side. She does most of the talking.
He’s spent a lifetime trying to make himself understood, and he’s found alternatives to the words that are so hard for him to shape. He uses his good eye and hand gestures to get his point across.
Two blocks from Grant, kids jam the streets. The wavy-haired girl subtly, discreetly, falls behind. When the boy slows to match her step, she hurries ahead. Sam lets her go and walks alone.
Grant, a great rectangular block of brick, looms in the distance. Every light in the place is on. Tonight, there are no shadows.
He arrives at the north door and stands on the steps, looking in through the windowpanes. Clusters of girls hug and laugh. Boys huddle under a sign announcing a basketball game.
Sam grabs the door handle, hesitates for the briefest of moments and pulls the door open. He steps inside.
He walks into noise and laughter and chaos, into the urgency that is all about being 14 years old.
Into a place where nothing is worse than being different.
* * *
The computer room in Sam’s house is out of main traffic patterns, and it’s a place where Sam can slip off into his own world. On the Internet, Sam is just another screen name in a chat room, where his words speak for themselves, unfiltered by his distorted voice or his appearance.
Years later she still wonders if it was something she missed, some sign that things weren’t right. But it wasn’t until her seventh month that Debbie Lightner learned something had gone terribly awry.
She struggled to sit up on the examination table. The baby, her doctor said, was larger than it should be. Debbie watched him wheel up a machine to measure the fetus. She felt his hands on her stomach.
“Something’s wrong,” the doctor said again.
He told Debbie he would call ahead to the hospital and schedule an ultrasound. He laughed and told Debbie he just wanted to be sure she wasn’t having twins.
The next morning, at the ultrasound lab, the technician got right to work.
He immediately ruled out twins.
Then, a few minutes into the test, the technician fell silent. He repeatedly pressed a button to take pictures of the images on the monitor. After 30 minutes, he turned off the machine, left the room and returned with his boss. The two studied the photographs.
They led the Lightners down the hall to a prenatal specialist. Their unborn child, he said, appeared to have a birth defect. The ultrasound indicated that the child’s brain was floating outside the body.
He had to be blunt. This child will die.
Some parents, he said, would choose to terminate.
No, Debbie remembers telling him. She and her husband were adamant that they would not kill this baby.
On Sunday, Oct. 6, 1985, six weeks before she was due, Debbie went into labor at home. David drove her to the hospital, and the staff rushed her to the delivery room for an emergency Caesarean.
She heard a baby cry. A boy. The boy they’d decided to name Sam.
She passed out.
When she came to, she asked to hold her child.
No, her husband said. The boy was in intensive care. He needed surgery.
David handed his wife two Polaroids a nurse had taken. A bulging growth covered the left side of the baby’s face and the area under his neck.
”What is it?“ Debbie asked.
“I don’t know,” David said. “But he’s alive.”
When the Lightners arrived at the neonatal ICU, they were led to an isolette, a covered crib, that regulates temperature and oxygen flow. A nurse had written “I am Sam; Sam I am”—a line from Green Eggs and Ham by Dr. Seuss—and taped it to the contraption.
Wires from a heart monitor snaked across the baby’s tiny chest. He was fragile, a nurse said, and they couldn’t hold him.
The mass fascinated Debbie, and she asked if she could touch her son.
The nurse lifted the cover of the isolette, and Debbie reached down with a finger. The mass was soft. It jiggled. Debbie thought it looked like Jell-O.
The nurse closed the cover.
Debbie and her husband returned to her room, and she climbed into bed. She picked up one of the pictures her husband had given her and covered the mass with her fingers to see what her son should have looked like. He had brown hair and eyes.
She wept.
* * *
The temptation is to break ranks during a family portrait, and wave when a neighbor drives by. Still almost everyone stays in character, Nathan, 9, is a cutup who mugs for the camera. Emily 12, tries to stay dignified. Maggie, the vocal family dog, is uncharacteristically quiet, but David and Debbie are their naturally casual selves.
Tim Campbell, a pediatric surgeon known for tackling tough cases, walked into the ICU and peered into the isolette. The boy had a vascular anomaly. They were rare enough, but what this tiny infant had was even rarer. The anomaly was a living mass of blood vessels. And it had invaded the left side of Sam’s face, replacing what should have been there with a terrible tangle of lymphatic and capillary cells.
The malformation extended from his ear to his chin. Campbell knew there was no way to simply slice it off, as if it were a wart, because it had burrowed its way deep inside Sam’s tissue. Doctors knew little about such anomalies except that they were made up of fluid-filled cysts and clots that varied in size from microscopic to as big as a fingertip.
Campbell gently pulled the baby’s mouth open. The mass swelled up from below and wormed its way into his tongue, threatening to block his air passage. He could barely breathe, and only immediate action would save him. He asked a nurse to direct him to the Lightner room.
Campbell introduced himself, explaining the surgery. He didn’t mince words.
“I’m going to be in there a long time,” the Lightners remember him saying. “It’s risky. He’s little, and he’s premature.”
Campbell operated for six hours and removed 1 pound, 10 ounces of tissue from under Sam’s neck. He operated a second time to remove bulk above his left ear and to ease his breathing with a tracheotomy tube. But there was no way, he told the Lightners, that he could safely remove the mass on Sam’s face.
Campbell had sliced away a quarter of the infant’s weight. Baby Sam, who weighed 5 pounds after the surgeries, spent three months recovering in the hospital.
* * *
He was 3 when he first realized he was different. His father remembers Sam running up and down a hallway when he stopped in midstride and stared at his image in a full-length mirror. He touched the left side of his face, almost as if to prove to himself that he was in fact that boy in the mirror.
He cried.
His parents had been expecting this day. His father bent over and took Sam by the hand. He led him to a bedroom off the hall. Debbie joined them. David lifted Sam onto the bed. And then his parents told the little boy the complicated facts of his life.
Except for the deformity, Sam was normal in every way. But everyone outside Sam’s circle of family and friends would have a hard time seeing beyond the mass of tissue on his face.
And so it was.
A little girl grabbed her mother’s hand when Debbie pushed Sam, in a stroller, onto an elevator. The girl stared at the little boy, pointed at him and then loudly told her mother to “look at the ugly baby.”
Bystanders often assumed Sam was retarded. A woman asked Debbie what drugs she had taken during her pregnancy. Strangers said they’d pray for the boy. Others just shook their heads and turned away.
His parents went to another surgeon to see if he could reduce the mass. He removed some tissue from behind Sam’s left ear but encountered heavy bleeding and closed up. Even then, the incisions wouldn’t heal. Sam bled for six weeks.
When the Lightners realized their son would have to live with his face, they refused to hide him from the world. They took him to the mall, to the beach, to restaurants. In Northeast Portland, where the Lightner family lived, people talked about seeing a strange-looking boy. “That boy,” they called him.
The Lightners enrolled Sam in the neighborhood school. Sam, his breathing labored, caused a stir during registration. Teachers worried about having the boy in their classes.
But he was an excellent student. He made friends, joined the Cub Scouts and played on a baseball team. He tried basketball for a year, but he fell easily because his head was so heavy.
When Sam turned 12, he told his parents that he wanted to change his face. They took him to Dr. Alan Seyfer, an OHSU professor who chaired the medical school’s department of plastic and reconstructive surgery. What Seyfer saw made him leery.
The mass was near vital nerves and blood vessels that surgery could destroy, leaving Sam with a paralyzed face. Hundreds of vessels ran through the deformed tissue, and every incision would cause terrible bleeding. Sam could bleed to death on the operating table.
Nonetheless, Seyfer, who spent 11 years as a Walter Reed Army Hospital surgeon, wanted to help. And so he scheduled Sam for surgery in June 1998. A month before he asked a friend, the chairman of the plastic-surgery department at Johns Hopkins Hospital in Baltimore, to join him.
A week before the surgery, Seyfer and his partner examined Sam one last time. They peered down his throat so they could study the mass without having to make an incision.
They didn’t like the view.
That afternoon, Seyfer met with Sam and his parents and said he had made an agonizing decision. The surgery was too risky. In good faith, he could not operate.
The news crushed Sam. He realized he had always held out hope that a surgeon would pull him out of the horrible spotlight that targeted him every time he went out in public. But no. He was trapped.
Graduation from eighth grade is a big night for Sam—he wins the citizenship award and receives a huge round of applause from the crowd of parents and students. Sam’s father playfully tousles his hair on the way out of the auditorium as brother Nathan watches.
Sam Lightner pedaled his bike as hard as he could, but his family zoomed ahead. His legs ached, and he panted for breath. Even his younger brother could ride his bike farther and longer.
Most days during this spring 1999 vacation, Sam wanted to just lie in bed and watch television.
And when he spoke, his family kept asking him to repeat himself. No one—the desk clerk at Central Oregon’s Sunriver Lodge, the woman in the gift shop—could understand him. He garbled his speech, as if he were speaking with a mouthful of food.
But he wasn’t eating. At dinner, he sat with his family, listening, picking at his food, waiting to go lie down on the sofa. Over his protests, his mother took him into the bathroom and weighed him.
Five pounds, she said. He’d lost five pounds. But a later visit to his pediatrician turned up nothing.
Sam woke up one morning in pain. He touched his face and found it tender. The mass was growing. His mother gave him Advil, but the mass continued to swell. Within a week, he couldn’t swallow the pill. He stuck his finger in his throat. His tongue felt bigger. By the end of the week, Sam cried continually.
A doctor removed a lump where Sam’s shoulder met his neck, thinking the lump was pressing against a nerve. But the pain continued.
On Sunday, Aug. 8, 1999, Sam came downstairs from his bedroom. He found his mother outside, sitting on the front porch. He walked out and sat next to her, crying. His speech slurred, and he had to repeat himself. The pain, he managed to tell her, had spread across the entire left side of his face.
The next morning, at the hospital, nurses poked and probed his face. He sat still while strange machines whirled about his head. And then he waited while specialists reviewed the X-rays and CAT scans. They found nothing.
Sam refused to go home. Someone, he pleaded, had to help him.
Doctors admitted him and ran more tests. Four days later, on Aug. 13, the mass awakened.
Pain racked Sam’s body. He tried to call for help but couldn’t speak. With his fingers, he reached up. His swollen tongue stuck several inches out of his mouth. He punched the button beside his pillow to call for help.
He wrote in a notebook to communicate with nurses and doctors, a notebook his mother would later store away with the other memorabilia of Sam’s medical journey.
“I have no idea why. Since I was a baby. I was born with this.”
“When I cough hard, little capillaries burst and a little blood comes out.”
“Don’t touch.”
“Please, it hurts.”
He held out his arm so nurses could give him morphine. They fed him through a tube.
Then the door to his room opened, and a new doctor walked in. The man asked Sam if he knew him. Sam shook his head.
“I’m Tim Campbell,” the doctor said.
He’d been making routine rounds when he spotted Sam’s name on the patient board. Campbell hadn’t seen the boy since he’d operated on him nearly 14 years before, the day after he was born.
Dr. Campbell thumbed through the reports at the nurses’ station. He checked Sam’s chart. The boy weighed 65 pounds—he was wasting away.
Campbell pulled up a chair.
“How do you feel?”
Sam wrote in his notebook: “Anything to stop the headaches.”
“Anything else?”
“I really don’t think this is going to work out.”
“The doctors are trying.”
“Please try your hardest.”
“Hang in there, Sambo.”
“I’m in pain. It was really bad this morning.”
Campbell made a note to order more morphine.
“I hurt.”
And methadone.
“I’m tired.”
“Try to sleep.”
“Will it kill me?”
The Boy Behind the Mask
Tom Hallman Jr.
Photos by Benjamin Brink The Oregonian October 2, 2000, Part 2
Acceptance sometimes comes in the struggle to achieve it
Dr. Tim Campbell looked down into Sam Lightner’s face. The boy, he remembers thinking, was giving up. Unless something dramatic happened, he would die.
Dr. Tim Campbell, the Portland surgeon who operated on Sam shortly after his birth, was on routine hospital rounds when he encountered his old patient and resumed caring for him.
The 14-year-old lay motionless in his bed at Portland’s Legacy Emanuel Hospital & Health Center. His bloated face spilled across most of the pillow. His tongue protruded grotesquely from his mouth, and the swelling on the left side of his face wrenched one eye completely out of position. In late summer of 1999, the deformity he’d carried since birth had suddenly grown to life-threatening size, choking off his airway and esophagus.
Sam, Campbell remembers thinking in blunt medical slang, was “circling the drain.” He’d seen the same look in children battling terminal cancer. At a certain point, they accepted their fate and surrendered to death.
The doctor hurried back to his office, rummaged through his desk drawers and pulled out a slim blue book, a list of every pediatric surgeon in North America. He flipped through the pages.
Campbell paused when he reached the résumé of Dr. Judah Folkman, a cancer researcher he’d met 30 years earlier when they were both young surgeons. Folkman’s research team had controlled tumors in mice by stifling the growth of the blood vessels that supplied them, causing a national stir and overwrought speculation that a cancer cure was at hand.
Folkman planned to test his technique on humans for the first time in May 1999. Campbell considered the fact that a wild excess of blood vessels had created Sam’s deformity. Maybe, he thought, Folkman’s strategy would work on the boy.
But Folkman, besieged by more than a thousand desperate cancer patients a week, is fiercely protective of his time. He grants no interviews. A secretary screens all calls.
Campbell punched in the telephone number listed in the blue book, hoping Folkman might grant a favor to an old friend. The secretary put him on hold. Then Folkman came on the line.
His response was discouraging. Sam’s malformation was fully formed, and his method worked only on growing tumors. But Folkman suggested Campbell call a pediatric surgeon who worked for him as a research fellow. Campbell scribbled out a name: Jennifer Marler.
She was a member of the Boston’s Children’s Hospital Vascular Anomalies Team, which treated malformations just like Sam’s. Pleas for help deluge that team, too, and the surgeons can respond to only a fraction. But when Campbell reached her, Folkman’s name provided instant access.
Marler suggested that Campbell take some photographs of Sam and send them along with the boy’s medical file. Campbell should address the package to her to make sure it didn’t get lost in the slush pile.
The best she could offer was that she’d take a look.
* * *
Sam Lightner turned his head and stared straight into the camera while Campbell photographed his face. After Campbell left the hospital room, a psychiatrist walked in, pulled up a chair and began asking questions. Sam scribbled his answers in the notebook he used to communicate.
Then Sam asked a question.
“Why is this happening?”
The psychiatrist had no answer. Instead, he asked another question. Tell me how you feel about life, Sam remembers him saying. Is life unfair?
How stupid, Sam thought. His tongue was sticking three inches out of his mouth. He couldn’t eat. His left eye bulged abnormally, reacting to pressure that seemed to build each hour. An IV drip line ran into his arm and pumped him full of drugs: morphine, methadone, Celebrex and nortriptyline—a combination of painkillers, anti-inflammatories and antidepressants. None of them helped. No one could tell him what was wrong.
Is life unfair?
“Sometimes.”
And then the swelling receded. Doctors couldn’t explain why, but the sudden eruption died down as mysteriously as it had come to life. On Sept. 2, 1999—after a month long hospital stay—Sam went home.
But everything was different. Physically, Sam was a shell. He had lost 17 pounds and was down to 63 pounds. He could not speak. And the battle with the malformation had scarred him. His mother remembers a listless child who wouldn’t stir from bed.
* * *
On Nov. 15, 1999, doctors determined Sam was healthy enough to get back into his old routine. When he returned to Gregory Heights Middle School, however, something had changed. All the talk in the hallways was about high school—girls, dances, sports. Being popular.
Life as Sam Lightner knew it was ending. All his classmates were obsessed with how they looked and how they fit in. But for Sam, the issues every young teen faces were magnified a thousandfold. He was moving out of the cocoon of familiarity that kept him among family and longtime classmates, who could see past the disfiguring mass he carried on his face. He was moving into a world of judgmental teen-agers and he would carry with him a terrible handicap, a face drastically shortchanged of its ability to reach others with a subtle expression, a slightly raised eyebrow, a flicker on the edge of his mouth. He was being cast among strangers who would turn away from his alien features so fast that they would miss the boy behind the mask.
Like all teens, Sam’s perception of how others saw him would determine how he saw himself.
And when strangers looked at Sam, they first fixated on the left side of his face, a swollen mass that looked like a pumpkin left in the fields after Halloween. His left ear was even more abnormal, a purple mass the size and shape of a pound of raw ground beef. His jaw, twisted. His teeth, crooked. His tongue, shoved to the side. His left eye, nearly swollen shut.
When he walked to school each morning, he stopped at the crosswalk on Northeast Sandy Boulevard and watched passengers in cars and buses stare at him. When he walked through the neighborhood, he heard laughter and comments.
Once, a neighbor boy led his friends over to Sam’s house and knocked on the front door so the others could see Sam’s face.
* * *
In late August, a thick envelope arrived in Dr.Jennifer Marler’s office. She noticed it was from a Dr. Tim Campbell, an unfamiliar name, and tossed it aside. At the end of the day, after a brutal round of surgery, clinics and lab research, she was about to head home to her husband and three children when she spotted the envelope.
She dropped into her chair, grabbed it, ripped it open along one end and dumped the contents onto her desk. She started with the medical report: Patient has lymphaticovenous malformation of the left side of face and neck. Condition was diagnosed prenatally. Involvement of the airway necessitated a tracheotomy. Difficulty swallowing necessitated a gastronomy tube. Malformation has grown to the point of orbitaldystopia. In all other areas of life, though, the patient has developed normally.
She remembered—the Portland boy.
She searched through the paperwork and foundseveral photos. She picked one up and held it between her fingers. The photograph haunted Marler.
The boy lay in a hospital bed, staring at the camera with pleading eyes. He looked like one of the children featured in ads aimed at raising money to help poor kids overseas.
Marler scanned the reports. The kid was on a morphine drip, diagnosed as clinically depressed.
Marler was 38 and had been a doctor for 11 years. Outside of a textbook, she had never come across such a profound facial deformity. He was the saddest-looking child she’d ever seen.
And she had seen many. A score of photographs hang on her office wall, the faces of children who have set the course of Jennifer Marler’s life. Some of the images show children she successfully operated on, relieving them of the deformities that robbed them of their futures. Others tell sadder stories, reminding her of children who died from their abnormalities or who took the risk of surgery and didn’t survive.
Marler picked up the telephone and spoke with the nurse who scheduled weekly team conferences for the Vascular Anomalies Team. During the meeting, doctors discuss cases and decide whether they want to tackle them. The nurse said the next chance to present a case would be Sept. 22, 1999, just three weeks away.
She decided she’d present Sam Lightner’s case and argue that he be brought to Boston. First, though, she had to get the facts down cold. She picked up the telephone again, called her husband, apologized and told him to have dinner without her. She talked to her three young daughters and told them Mommy had something important to do.
* * *
The team met Wednesday evenings in the surgical library. Members, fellows and residents gathered around a 15-foot-long oak table, nibbling cookies and sipping soft drinks.
Everyone found a seat, the lights dimmed and the patients’ images appeared, one by one, on an overhead screen. The team members flipped through paperwork, scanning each patient’s medical history. They spoke in short, clipped sentences, rife with medical jargon, challenging one another, looking for potential problems that might rule out surgery.
Marler remembers studying the paper in front of her. Nineteen children were up for consideration. Fewer than half would be chosen.
The team moved quickly: The agenda included an 8-month-old girl from Argentina. A 3-year-old girl from Italy. A 9-year-old boy from Minnesota.
Sam Lightner was next. His picture—the one Dr. Tim Campbell had taken—flashed on the screen.
“Who is he?” someone asked.
Marler recalls choosing her words carefully. She wanted to make sure the team knew something of the boy’s life. He was in pain, she says she told them. Without hope. The disfigurement severe.
Although the center takes some of the most difficult cases in the world, Marler knew Sam Lightner presented major problems.
Behind her, she heard papers rustle as the team read his medical history. They quickly zeroed in on those risks. They hesitated. Before making any decision, the team members wanted more information.
Next case.
Marler scheduled Sam for the Nov. 3, 1999, meeting. Again the answer was no.
At the Nov. 10 meeting, she tried again, focusing not on the entire team, but on Dr. John Mulliken, the surgeon who directs the Vascular Anomalies Team and a researcher who’s trying to figure out the causes of defects such as Sam’s. Mulliken lectures at hospitals around the world and co-founded the International Society for the Study of Vascular Anomalies. He’s written 185 scientific articles, 40 book chapters and two complete books.
The way Marler saw it, a team of doctors would have to operate on Sam. And Marler wanted to be on the team.
At this meeting, she spent an unusual 30 minutes arguing her case, knowing this was her last chance. She studied Mulliken, an impatient man, as he reviewed the files. She knew what he was thinking—the horrendous bleeding, and the tangle of nerves in the mass. If Mulliken damaged one, the boy might lose the ability to speak, to close his left eye or to smile.
She appealed to Mulliken’s pride and compassion. No other surgeons, Marler remembers telling him, believe they can fix this.
She watched Mulliken, Sam’s last hope.
The projector’s motor hummed. Sam Lightner’s face peered out into the room. Mulliken looked up at that face.
Bring him to Boston, he said.
* * *
Sam, on his first commercial airline flight, checks out a map and discusses it with his mom while their MD-80 carries them across the country to Boston, where Sam will meet the surgeons at Children’s Hospital.
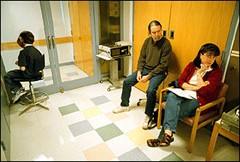
The visit to Children’s Hospital includes a long round of appointments with different doctors In one waiting room, Sam entertains himself by spinning in an office chair while his parents mark the hours.
On April 7, 2000, Sam Lightner and his parents walked three blocks from their Boston hotel to Children’s Hospital. The Lightners silently rode an elevator to the third floor, where a smiling receptionist waved them over and took the Lightner file. Sam found a seat and flipped through a stack of magazines. He caught the eye of a woman sitting across from him. She turned away. Sam saw her whisper something to a woman sitting next to her before both turned back to stare.
“Samuel Lightner,” the receptionist called.
A woman led them down a hallway to an examination room. Sam climbed onto the table. A few minutes later, the Lightners heard a soft knock.
She stood 5 feet 7 inches tall and wore a white doctor’s smock over a long black skirt with matching black hose and shoes. Her brown hair was cut in a pageboy. “I’m Dr. Marler,” she said.
She sat down on a doctor’s stool, tugged on her glasses and fiddled with a string of pearls that lay across her white and blue-striped blouse. “I’m so glad to meet you,” she told Sam. A flush spread up his neck.
Debbie Lightner dug through her purse and handed Marler a picture taken shortly after Sam’s premature birth. Marler stared at the image of the tiny infant. “Boy,” she said, “you were a little peanut.”
The Lightners explained Sam’s medical history—the emergency surgery right after his birth, the ear surgery that led to six weeks of persistent bleeding and the reluctance of other surgeons to even attempt cutting away the main mass of tissue. Marler took notes, interrupting occasionally to ask a question or to look at additional photos.
“I think you’re in the right place,” she continued. “Dr. Mulliken is both a craniofacial surgeon and a specialist in vascular anomalies. That makes him the right man for the job.” She swiveled to face the examination table.
“So let’s take a look, Sam.” She patted his knee. He smiled.
“What grade are you in now?”
“Eighth,” he said, in his raspy voice.
Marler ran her fingers across the mass, sizing it up. She sighed.
Sam’s father cleared his throat. “He’s going into the ninth grade,” David Lightner said. “He wants the size of his head made smaller. He’s a little bit more concerned about his appearance now.” Marler patted Sam on the shoulder. “I can understand that, Sam,” she said. “I’ll bring in Dr. Mulliken and our cast of thousands. On this one, we’re going to need everyone’s opinion.”
She walked out, closing the door after her.
“You’ve been waiting for this a long time, haven’t you, Sam?” Debbie Lightner asked her son.
“Nervous?” his father asked.
“I’m just hoping.”
The door opened, and Marler walked back in, followed by six doctors who formed a semicircle around Sam. A man wearing a bow tie with blue and red polka dots stepped forward.
“Hi, Sam. I’m Dr. Mulliken. Nice to see you.”
He perched on the examination table next to Sam. He took the boy’s head in his hands as if holding a basketball and moved it gently, running his fingers from one side of the face to the other. He frowned. All the blue veins showing through Sam’s waxen skin worried him.
“Oh, boy,” he said. “There’s a lot of venous component there. This is an incredible overgrowth.”
He released Sam’s head and climbed off the examination table. He stepped back two feet and crossed his arms, looking like a sculptor studying a block of granite. He moved to the left. The semicircle moved with him. Back to the right. The other doctors shuffled into place.
Mulliken ran his hands over his face. He groaned.
Marler jumped in. “I think he has very good facial nerve function.”
“Smile, Sam,” Mulliken commanded.
He sighed again. “OK,” Mulliken said. “Let’s write down some things.”
That was what Marler had waited eight months to hear. She smiled, sat on a stool and opened her notebook, ready to send off instructions on what Mulliken needed to know about the inside of Sam Lightner’s head.
“I want Reza to look down the trach and see what’s going on there,” Mulliken said, asking one of his colleagues to peer down Sam’s airway. “Send him to AP for a Panorex. Find a CP and get pictures downstairs. We’re going to have to decide what’s going on in terms of flow, and if there’s anything we can do to make it easier.” He looked at Marler.
“Got all that?”
“Right,” Marler said.
Mulliken boosted himself back onto the exam table. He scooted up next to Sam as if he were the boy’s grandfather. He put his hand on Sam’s knee.
“What bothers you the most?” he asked. “If you had one thing you wanted, what would that be?”
Sam shrugged. He stared at his hands, folded in his lap.
“Should I give you some choices?” Mulliken asked. “Some multiple choices?”
Sam responded with a barely perceptible nod.
“Our goal will be to make you look as symmetrical as possible, to balance out your face,” he said. “A Picasso is a great painting, but no one wants to walk around with one for a face. We have many things to talk about: Making your ear smaller, the tongue movement, the eye. The neck’s pretty good.”
He put his arm around Sam’s shoulder. “What do you want, Sam?” he asked quietly, as if the room were empty except for the two of them.
Sam bowed his head and stared at his hands.
“Well, you’re really down to the choice of two things,” Mulliken said. “We can focus on the face or the ear, but we can’t do both at the same time. If we get the face smaller, the ear will look bigger. Frankly, I just don’t know. The face is tough, very tough. Lord, I just can’t imagine…”
Sam raised his head. He looked deeply into Mulliken’s face with his one good eye. “I want to fit in,” he said in his raspy whisper. “I want to look better.”
Mulliken nodded, his features softening. He pulled the boy a little closer. “I can understand, Sam.”
David Lightner, standing against the back wall, pushed his way through the semicircle until he faced Mulliken, who dropped his arm from Sam’s shoulders and faced the father. “His goal?” Lightner said. “Well, Sam’s 14 years old. Like you put it, he’d like a more symmetrical face. I’m ambivalent. I understand the risk of the whole thing. But this is something Sam wants. We’re supporting him.”
“OK, Dad,” Mulliken said. Then he swiveled on the table and faced the doctors.
“I think it will be reasonable to focus on this huge area on the side of his face,” Mulliken said. “It’s no-man’s land, and it will be hard to work in that area. The problem’s going to be finding the facial nerve branches and separating them from the malformation. They look exactly alike.”
Mulliken slid off the table and paced. He shook his head, as if he were having an argument with himself. “The bleeding. Boy! When you are dealing with a pure lymphatic tissue malformation, bleeding is just an annoyance. But if you have these venous components, which he has, it’s more than a problem.”
He smiled. “But Sam, I’m going to try.”
The goal, Mulliken told the room, was to get the mass on the side of Sam’s face down to the bone. If Mulliken could eliminate the mass, Sam could return to the hospital for more surgery to reshape the bone. That surgery would be much easier.
Dr. Jennifer Marler (left) acted as Sam’s persistent advocate, urging her colleagues to bring him to Boston. There, Dr. John Mulliken got his first look at the Portland boy.
“Another operation?” Debbie Lightner asked. “The insurance company’s going to really love us.”
Mulliken broke through the semicircle and stopped in front of her. “Listen,” he said, “you show that insurance company photographs of this boy and there won’t be a dry eye in the house.”
The Lightners looked at each other.
Mulliken moved aside so they could look at Sam.
“Sam?” his father asked.
Sam nodded, more firmly this time.
Mulliken moved back to his patient. “This is going to be tough. We’re in for a rough time in the operating room. It’s going to be a microscopic dissection, and we’re going to need a team.”
He looked around the room. “Dr. Marler, me and one or two others.”
He stepped back once more to look at Sam. “His face is going to be swollen for a long time,” Mulliken said. “By the time he goes to school, though, he should look considerably better. Push me to the wall, and I’d like to think we could make it 50 percent better.”
“Sam,” he asked, “is this something you really want?” Sam nodded. Mulliken patted the boy on the shoulder.
“Let’s schedule for July,” he told Marler.
Sam’s father cleared his throat. “From seeing him in person, is this something you want to do?”
3-D CAT scans revealed the extent of the bone deformity that lies beneath the tissue mass on Sam’s face. The shape of the bone means that Sam’s image will remain distorted even if the tissue mass is removed, although surgeons think they can straighten the bone in a later—and much simpler—operation.
Mulliken frowned. “Well …”
“I’m being blunt,” David said. “We have to know.”
Mulliken sat on the exam table again. “I don’t know if ’want’ is quite the right word,” he said quietly. “I think that we can do it.”
He ran his hands over his face. “I know we can do it,” he said. “I wish I could make him perfect. All plastic surgeons search for perfection, just like Michelangelo. I can’t give him perfection.”
He hoped he could remove a large amount of tissue from the side of Sam’s face. But he also knew the underlying bone would remain seriously misshapen. When the world looked at Sam after the first surgery, it would still see an extraordinary deformity. But removing the tissue was the necessary first step to dealing with the bone.
“Dad, I’m bothered that he has to live with this mass,” Mulliken said. “Everyone should have the right to look human.”
* * *
Doctors worry about the nerve function in Sam’s face, and they check carefully to see how his deformity has affected his ability to feel and move.
The giddiness the Lightners felt vanished almost as soon as the jet roared down the runway at Logan International Airport and headed west, back to Portland, back to reality. Once home, David and Debbie went back to work, and Sam returned to eighth grade.
Sam’s mother took Sam to register at Grant High School. An administrator walked in, noticed the Lightners sitting outside the counselors’ office and stopped. He introduced himself and shook Sam’s hand. He turned away from the boy, as if Sam were deaf. He told Debbie that Grant had a great special-education class for mentally retarded students.
Her son, he said, would love it.
* * *
The telephone rang in the Lightner home. Dr. Jennifer Marler told Debbie Lightner that surgery was scheduled for July 6. Having a date, something to put on the calendar, made it real. And frightening.
After dinner, the Lightners called their children together. Sam sat at one end of the dining-room table, his father at the other. In between were Debbie, Emily, 12, and Nathan, 9. The family cat, Alice, jumped onto the table.
David Lightner played with a pencil, turning it end over end. “I wanted to discuss how this is going to affect us,” he said. “We’re up in the air about whether we should do it. Mommy talked with Dr. Marler for quite a while. There are dangers, but Dr. Marler said if Sam was her child, Dr. Mulliken would be the man.”
David fiddled with a magazine. “There are some things that could happen,” he said. “We have to be honest about that.”
“Like what?” Nathan asked.
“If some of the nerves are damaged, Sam’s face could droop,” his mother said. “He’d be paralyzed on that side.”
“You mean he wouldn’t feel it?” Emily asked.
“Right.”
No one looked at Sam.
“He might bleed a lot during surgery,” his mother said. “They think they can control it, but you never know. I think Dad just wanted to have it all out on the table for everyone to talk about one last time.”
David Lightner shifted in his chair.
“Now that we’re 3,000 miles away,” he said, “it puts a different spin on it. It’s more complicated sitting here.”
Debbie touched Sam’s arm. “Sam, do you still want to do this?”
Sam nodded.
“I want to hear it.”
“Yes,” Sam said, firmly.
“It’s your decision,” his father said. “That’s the deal. If I felt something was wrong, I’d intervene. I don’t sense that. But I have to be honest, it scares me a little bit.”
“Me, too,” Nathan said.
“Me, too,” Emily said.
“I worry about the potential damage to him,” said David. “As it stands, he’s Sam. He is who he is.”
“He’ll look different,” Emily said. “Sam is Sam.”
“He is who he is,” said David. “We don’t think anything’s wrong with him.”
David leaned forward, arms on the table, and stared across at his son. “Any doubts, Sam?” he asked. “If you say ’no,’ we call and cancel right now, date or no date.”
“I’m a little nervous,” Sam said. “But I like the doctors.”
“Well, it scares me,” his father said. “It’s the unknown. Here we have the situation that Sam deals with. It’s the known. It’s not ideal for him because of his face. His face freaks people out. But it’s a known property. And it’s a little bit scary to risk everything because the world doesn’t accept his face.”
“Dad, I’m sure,” Sam said. “Look what happened at Grant.”
His father bowed his head.
“That’s what people think about him,” Debbie said. “They think he’s mentally defective.”
Sam leaned forward and mustered all his strength.
“I want to do this,” he said.
David placed both hands on the table.
“We are fearfully and wonderfully made,” he told his family. “And very fragile.”
He sighed.
“All right,” he said. “It’s a go.”
The Boy Behind the Mask
Tom Hallman Jr.
Photos by Benjamin Brink The Oregonian October 3, 2000, Part 3
The risks we take can tell us who we are
A nurse appears in the doorway. It’s time to go, she says. Sam Lightner takes a deep breath and nods feebly. He lifts himself, his hands trembling slightly on the arms of the chair, and walks across the small pre-op waiting room to give his parents a hug.
“We love you, sweetie,” says his mother. She pulls him close and kisses him softly on his left cheek, right on the mass that the waiting team of doctors will target. Sam looks at his mother through his right eye—the only truly normal feature on his face. He blinks it once. A wink.
“Have a nice sleep,” says his father as he gives his son a hearty pat on his shoulder.
David Lightner wraps his arms around his son as a nurse waits to walk Sam down the hallway toward the operating room.
The nurse touches the 14-year-old on the shoulder and leads him down the hallway. His gown hangs loosely on his 83 pounds, exposing his spindly legs. In another room, nurses help him onto an operating table. He lies down, and a nurse inserts an IV line into an arm. Then she injects drugs to make him drowsy. When his eyes flutter, he’s wheeled into Operating Room 16.
It is Thursday, July 6, 2000, just three months since Sam and his parents visited Boston to find out if this elite surgical team, the only one in the world with any chance of correcting his deformity, would take his case.
The room is about the size of a two-car garage with a 15-foot ceiling. It’s chilled to 64 degrees, which cuts down on the growth of germs and keeps the doctors comfortable as they work. Two massive operating lights, each with four bulbs, hang over the table. Everything but the white walls—the drapes that cover the patient and the operating table, the surgical scrubs and the shoe covers—is light blue.
“You’re just falling asleep now, Sam,” says a nurse as she strokes his hair. “Just falling asleep, Sam.”
His eyes close.
An anesthesiologist takes her place behind the bank of machines that will control the boy’s body during the operation. She switches a knob, and the sound of a pump fills the room. It is a steady beat—one swoosh every two seconds—and fills Sam’s lungs with air, breathing for the unconscious boy.
The circulating nurse, responsible for everything that comes in and out of the room, sorts through a cluttered desk to find Sam’s medical history. In these final quiet moments, she sits on a corner stool and flips through a folder the size of a small telephone book, reading about this small boy’s long journey. The nurse puts the file down and walks to the operating table. An intravenous line pumps Sam’s body full of saline, a way of making up blood volume in the face of the bleeding that is sure to follow.
A member of the medical team comforts Sam as he lies on a gurney, drifting off into anesthetic sleep in the moments before the surgery begins.
The swinging door to the scrub room opens with a bang, and Dr. Jennifer Marler enters Operating Room 16. Her arms drip with water. The circulating nurse hands her a sterilized towel.
Marler, a 38-year-old mother of three, lobbied to bring Sam here to Boston, to Children’s Hospital, the nation’s largest pediatric medical center. In late 1999, Marler presented and pressed Sam’s case before the hospital’s Vascular Anomalies Team. The team members balked—the surgery was tremendously risky. But eventually Marler won them over.
The goal was to cut away a mass on the left side of the boy’s face. If all goes well, that will set the stage for a later operation on the misshapen bones in his face. But first, surgeons must cut their way down to the facial bone.
A nurse helps Marler into her surgical gown and a set of gloves. She moves to the operating table. She runs her hands across Sam’s face, gently, almost caressing the boy, not as a doctor but as a mother.
“We’ll take good care of you, Sam.”
She leans over his body and begins suturing his eyelids. She does not want his eyes to open during surgery—the swirl of scalpels, needles and surgical gowns around his face could scratch a cornea.
Word about Sam and the impending operation has filtered through the hospital, Harvard Medical School’s primary pediatric teaching hospital. The staff is curious about something that pushes the boundaries of medical practice.
A nurse from Operating Room 17 pops in. “Wow,” she says. “How old is he?”
“Fourteen,” says Marler.
“Where’s he from?”
“Oregon.”
“Does he go to school?”
“He does,” says Marler. “He’s very personable.””
As Marler begins preparing Sam’s face, the scrub doors swing open, and Dr. John Mulliken, the surgeon who will lead the team, strides silently into the room. He stops to study Sam’s three-dimensional CAT scans, which hang from a lighted viewing board. He has never encountered so complex a case.
He holds out his hands. A nurse helps him into his gown and gloves. He walks to the operating table and looks at his patient. “Good preparation,” he tells Marler. “Good preparation.”
Surgery is Mulliken’s life. He works weekends. He hasn’t had a vacation in years. He’s never married and has no children. He dotes on his dog, Girlie, and his cat, Felicia. A cabinet in the operating room carries 19 photographs of the two pets.
During surgery Mulliken can be gruff, and some of the rotating nurses have complained to the administration that he barked at them when they didn’t move quickly enough or when they handed him instruments he didn’t consider clean. But for this operation, Mulliken has assembled a team of people who have worked with him for years. They all have thick skins.
He reaches down and grabs Sam’s head with both hands. “His head’s just so big,” he mutters. “It just rolls around.”
He turns to a nurse. “I can’t have it rolling,” he says. “Stop it.”
The nurse scurries through the room, searching in cabinets until she finds something that looks like a doughnut the size of a dinner plate. Sam’s head fits in the hole. Mulliken tries moving the head. It doesn’t budge. “Good,” he says.
The swinging doors open again. Dr. Gary Rogers joins Mulliken at the head of the operating table. The blue surgical scrubs cover their bodies. The caps fit snugly over their heads. Masks hide their mouths and noses. Each wears special black glasses outfitted with surgical microscopes that will allow them to peer deep into the boy lying in front of them.
Mulliken ignores his teammates. He walks around Sam’s head, studying it from all angles. Knowing this would be a difficult operation, he had scheduled a warm-up earlier in the morning: repairing a cleft palate in an infant. His hands are limber and steady.
The surgical nurse makes the final adjustments to tool-lined trays beside her. The circulating room nurse awaits her first order. Mulliken, Rogers and Marler adjust the microscopes over their eyes. Mulliken points to a spot near Sam’s left ear. That, he says, is where he wants to make the first cut.
“Everyone agree?”
Marler and Rogers bend over Sam. “Yes,” they say in unison.
Mulliken takes a deep breath. “OK,” he says.
He holds out his right hand and asks for a scalpel. He grasps it firmly. “This is going to be a bear,” he says. “Let’s do it.”
The scalpel parts the skin, and the flesh gives way to the blade.
Then the blood begins to flow.
* * *
Bathed in the intense glow of the operating-room lights, Dr. John Mulliken (left) and Dr. Jennifer Marler (right) struggle to find the facial nerves hidden in the mass of tissue they are trying to remove from Sam’s face.
The first drop of blood lands on the floor, and Mulliken calls for suctioning. Marler uses a tool attached to a clear plastic tube. In seconds, it resembles a piece of red licorice that snakes across Sam’s body, down the floor and to a holding tank where the boy’s blood collects.
Rogers holds back the skin, allowing Mulliken to proceed. After 15 minutes, the lead surgeon has opened up a 3-inch incision. The bleeding hasn’t slowed.
He calls for a syringe. Marler injects more drugs designed to speed clotting into Sam’s neck, hoping they will slow the bleeding.
The team waits. The blood flows freely.
The team confers. Mulliken could close up now, suture the incision and end the operation. When the Lightner family traveled to Boston three months earlier to meet Mulliken and Marler, Mulliken made it clear that this surgery was risky. The only other time Mulliken tackled a case this serious, he made an incision, encountered massive bleeding and closed.
If he continues, he and his team will have to work furiously, trying to stay one step ahead of massive bleeding while they peel back the skin. And even if they expose the mass, they might never find the nerves that branch out into the tissue. If they cut a nerve, they could paralyze the left side of Sam’s face.
The tissue mass is a jumble of skin, tissue, nerves, lymphatic vessels, veins and arteries. A Nerf ball filled with blood and fluid. Mulliken has no road map. If he plunges ahead, it will be like replumbing a house with the water turned on.
Operating Room 16 awaits his decision.
He leans over Sam’s body. “Let’s do it,” he finally says.
The circulating nurse jumps from her chair and hustles to a phone. She punches in the four-digit number to the hospital’s blood bank. Six units of blood are now in a cooler in Operating Room 16. The nurse tells the bank to set aside an additional six. Even if all goes well, Sam will bleed so much during the operation that she will have to replace his entire blood supply.
She glances to a plastic bag holding a unit of blood that drips from an IV line into Sam’s right arm. The bag is half-empty.
Mulliken lengthens the incision. The bag drains.
Mulliken, Marler and Rogers operate quickly, the suctioning line thick with the boy’s blood. Each time the scalpel moves, it slices a blood vessel. They go through 50 surgical towels and countless sponges, soaking up blood so they can see where they are.
Mulliken calls for the Bovie, a machine that electrically cauterizes blood vessels. In a normal body, the machine stops bleeding, and the surgery is almost bloodless. Marler leans over Sam’s body and grasps the Bovie, a device that looks like a dental drill, in her right hand.
There is the sound of sizzling, as if grease has been dropped onto a grill. A plume of smoke rises from Sam’s face. But the bleeding continues.
A nurse walks behind the surgical team and hangs a third bag of blood on the IV line. “Jesus Christ,” Mulliken mutters.
The team begins to pull back the skin. They can see the edge of the mass. “Easy,” Mulliken tells Marler. “Easy.”
The side of the boy’s face oozes blood. Drops splatter the floor. A red stain spreads through the surgical drape as if someone had spilled a glass of wine on a white tablecloth. Nurses call for another 10 towels. Within minutes, they are soaked through, and the nurses dump them into a bucket.
The insides of Marler’s shoes are soaked with Sam’s blood. She asks for a new pair of wool socks.
Mulliken sees only one option: They’re going to have to stitch each blood vessel closed. He calls for needles.
While Marler continues cutting, Rogers uses the Bovie, and Mulliken starts stitching. The surgical nurse goes through packet after packet of stitches and tells the circulating room nurse she needs more.
Mulliken’s fingers tire, and Marler takes over. Then Rogers. The bleeding slows to a trickle. The team has tied more than 200 stitches.
Slowly, they pull Sam’s skin back and cover it with a towel to keep it moist.
The mass is exposed.
Mulliken looks to a board in the far corner of Operating Room 16. Sam has gone through three units of blood. And the team hasn’t even reached the heart of the operation. He steps away from the table. He tells Marler and Rogers to clean up the area surrounding the mass. He’s going to take a break.
The phone rings, and the circulating nurse answers it. “We’re No. 1 again,” she calls out to the room.
For the past 10 years, U.S. News and World Report magazine has ranked Children’s Hospital best in the country. It’s won the award again.
“Your friend says you had a bet with him,” she tells Mulliken. “He says you owe him a dinner. He wants lobster.”
Mulliken strolls toward the door. “Yeah, yeah, yeah,” he says, disappearing through the swinging doors.
* * *
Surgical coverings hide Sam’s body and most of his face, leaving only the tissue mass exposed under the glare of the surgical lights. It looks like a piece of raw prime rib.
Even to someone as experienced as Mulliken, the mass is a mystery. X-rays don’t show soft tissue. So there’s no way of knowing how invasive the mass is or what it’s wrapped around. A single nerve leaves the brain and divides into five branches that spread out to control the side of the face. But the mass could rest on top of nerves, or it could spread under them. Or the nerves could snake right through it.
The boy has few enough pathways to connect him with the rest of the world. If Mulliken guesses wrong and cuts a nerve, Sam loses an important part of what he has left—the ability to blink his eye, to crinkle his forehead or to smile.
News of what’s going on in Operating Room 16 has spread throughout the third floor. Residents and other doctors wander in to look at the CAT scans hanging on the wall. They stand back and stare at the mass, bloody and glistening in the high-powered lights.
“Unbelievable,” says a visiting doctor.
He turns to the circulating nurse. “How old is he?”
“Fourteen,” she says. “And he’s really nice.”
The doctor looks at scans, which make Sam look like a cyborg in a science-fiction movie.
“Isn’t that the saddest thing you’ve ever seen?” he asks. “It’s heartbreaking. This kid must have a tough life. That’s no way to live.”
On the way out of the room, he passes Mulliken, who re-enters Operating Room 16 with a shout. “Children’s Hospital is tops,” he says. “We’re No. 1.” Even through his surgical mask it’s clear he is frowning.
“I was hoping we would be second or third,” he announces. “That way we won’t be so damn complacent around here.”
He checks with Marler. The blood has slowed to a trickle.
His job now will be to hunt for the nerve branches and to cut away the mass of tissue. The team will use an electric probe. If they touch a nerve, a portion of Sam’s face will twitch.
Out of habit the circulating nurse pulls down a thick anatomy book. She turns to the page that details the facial nerves and leaves it open on a table so the team can refer to it. But it will do them no good. In this section of Sam’s body, nothing is where it should be.
The team works under microscopes. Looking for the nerve will be like hunting for a white rope encased in white concrete.
Test. Cut. Test. Cut.
They begin removing bits of the mass. The bleeding begins again.
An hour passes, and Mulliken goes to the scrub room. He takes off his gown and gloves, and returns to flop in a chair away from the operating table. The pressure is intense, physically and mentally, and the team plans on working shifts—when one surgeon tires another will take the scalpel. Mulliken leans back and rests his head on a cabinet. He closes his eyes. After 15 minutes, he stirs.
“How’s it going,” he calls to Marler.
“The nerve must be surrounded by scars from his previous surgery,” she says.
“Don’t relax,” he tells her. He knows the biggest danger is in getting sloppy and cutting something that appears to be tissue but may in fact be the edge of a hidden nerve.
“Jennifer, are you looking?”
“There’s nothing,” she tells him.
He leaves the room to scrub and to check on his cleft-palate patient. He returns 30 minutes later. About four and a half hours have passed since the surgery began.
“How you guys doing?” he yells when he enters Operating Room 16. The silence is ominous. After getting in his gown and gloves, he moves to Marler’s side. He looks over her shoulder.
“Is this the same case?” he jokes.
“Hey,” she admonishes him with a chuckle.
“You found it yet?”
“We think we found the region.”
“I know the region,” he says. “I want the nerve. Where is it?”
He takes over, and Marler strips off her gown. She is going to take a shower, get something to eat and call her family and tell them she won’t be home until late that night.
Test. Cut. Test. Cut.
A nurse walks behind the surgical team and hooks up a fourth unit of blood to Sam’s IV line. Marler returns 20 minutes after leaving and finds Mulliken frustrated and worried. They haven’t found any branches of the main nerve, and the operation is entering its fifth hour.
And the kid is bleeding. He thinks of Dr. Alan Seyfer, the Portland surgeon who nearly attempted a similar operation on Sam when the boy was 12, and then decided the risks were simply too great.
“Seyfer was right,” Mulliken grumbles. “Seyfer was right.”
He mops up more blood and turns to see that the fourth unit is nearly gone. “This was a mistake to take this case,” he says. “I don’t think we can help this boy.”
Mulliken tells his team there are two choices: Increase the risk of destroying part of the nerve by cutting even faster. Or close up.
“I’ve been here before,” he says. “I think we should close up.”
Marler turns to him. “Let’s keep going.”
Mulliken moves to the side. “Jennifer,” he snaps, “you take over. You wanted to bring him here; you look for the nerve.”
Marler takes the probe, and 90 more minutes pass. The team has gone through more than 200 sponges and towels soaking up Sam’s blood. The holding tank where the suction line empties sloshes red.
“I think I got it,” Marler shouts.
“This is in a portion of scar tissue like you have never seen,” she tells Mulliken, who pats her on the back.
She applies the electric probe again, and a muscle twitches. “You got it?” Mulliken asks.
“I got it,” says Marler. “It’s all encapsulated. I can’t distinguish the nerve from the scar tissue. And it’s deeper than it should be. I’m afraid to dissect any farther.”
Mulliken trades places with her. He peers into the side of Sam’s face and holds out his right hand. A nurse hands him a scalpel. He leans over, inches from the mass. He touches it with the tip of his scalpel.
“Well, I can’t budge it from the scar tissue,” he says. “It is literally entangled in it.”
Marler uses the probe. Sam’s forehead moves.
“Every time I dissect, I’m worried,” Marler says. She and Mulliken turn away from Sam and look intently at each other.
“It’s bad,” he says. He peers back into the mass, which is oozing blood. He stands up.
“We’ve come this far,” he says. “We’ve got to get it out.””
Rogers assists with suctioning and controlling the bleeding so Mulliken can see where the nerve might lie.
“Let’s stimulate around what we think is the edge,” Mulliken says.
Test. Nothing. Test. Nothing. Test. Reaction.
Mulliken cuts. “It should be under here,” he says. “Jesus.”
He sighs. “I would go right here,” he says.
Mulliken, Marler and Rogers, instruments in each hand, all focus on a spot in the mass the size of a quarter. “I think I found a branch above,” Mulliken says.
The fourth bag of blood is nearly gone.
Mulliken turns to Marler and asks for the probe. He tries to work his way back up the tiny nerve he’s located, searching for the main branch.
He applies the probe again, but the room is silent.
“Come on, people,” he snaps. “Talk to me.”
“Yes,” says Marler. “His forehead moved.”
Mulliken tries again. They are more than six hours into the operation.
“Bingo,” says Mulliken.
* * *
The surgery has dragged on for hours with little progress, and Mulliken, taking a breather next to an array of Sam’s CAT scans, is feeling the frustration and exhaustion.
Darkness has fallen and more the 10 hours of surgery have already passed as David and Debbie Lightner doze in the empty waiting room.
The team moves out from the nerve they’ve located, hunting for other branches. “We have to see it, to get around it,” Mulliken says. “The nerve is going right through this mass.”
Marler turns to him. “Just imagine what it’s going to be like getting there,” she says. “What are we going to do?” Mulliken says nothing.
“Could we get the malformation off and then go back and do a nerve graft?” she asks.
“No,” he says. “We can’t even find all the nerves. Jesus Christ,” he says. “We’ve been here nearly seven hours, and we can’t even get to the nerves.”
Rogers strips off his gown and leaves the room for a break. Mulliken and Marler bend over Sam. Suddenly, blood spurts onto Marler’s blue gown. The scalpel has nicked a branch of the carotid artery.
“Bleeder,” Mulliken yells, calling for clamps and sutures to stanch the spurting blood. The surgical nurse doesn’t move fast enough for him. “Come on,” he shouts. “Come on.”
He works frantically. “We got a real bleeder here,” Mulliken yells. “Oh, Jesus.”
The fourth bag of blood is gone. A nurse scurries to hang a fifth, which drains as though it has a hole in it. A sixth bag begins to empty just as fast.
The blood loss could send Sam Lightner into cardiac arrest. He is close to death.
Mulliken leans into Sam’s body, violently shifting the head, stitching and then reaching out to grab another instrument and stitching again. The bleeding slows.
Rogers returns. “What’s up?” he asks.
“We get into the carotid branch of the vessel, and you walk off?” Mulliken says.
Rogers, mystified, looks at Marler.
“We’re fine,” she says. “We’re fine.”
* * *
The hallway outside Operating Room 16 empties. It’s 10:30 p.m., and janitors are already cleaning the surrounding rooms, readying them for the next day’s cases. In all of Children’s Hospital, only one surgery continues—the one in Operating Room 16.
The members of the team have to get reoriented. They suction off the blood and begin testing, looking for nerves again. Mulliken probes. “Let’s get going here,” he says. “We’re losing time.”
He asks the surgical nurse for a tool covered with green dye and maps the nerve branches right on the exposed tissue. The team can cut anything in between the green lines. When they reach the edge, they must test, getting as close to the nerve as possible. They think they’ve found all the nerves, but they won’t be sure until Sam regains consciousness and actually tries to move.
They begin cutting.
Small pieces, the size of a toenail clipping. Then much larger, some of them size of a marble. “Say,” Mulliken says. “You know that we’re the No. 1 hospital in the country?” He chuckles.
Nurses and doctors laugh.
“You know what we are doing now?” he asks. “We’re rolling, rolling, rolling.” He sings lines from the theme to the old television show “Rawhide.” And hacks away at the mass.
“You ever see anything like this?” one nurse asks another.
Marler dissects the area under Sam’s chin. “That should go,” she says as she pulls out a large chunk. “Let’s go the extra mile.”
Mulliken pulls the flap of skin back over Sam’s face. “He looks a lot better,” he says.
He folds the flap back down. “Folks,” he says, “We’re down to the bone.”
* * *
Sam’s blood has completely lost the ability to clot, and the nurse rushes to replenish it with a seventh bag. “He’s bleeding from every little hole,” Mulliken says. “Jesus Christ, things are starting to blow up. We’re getting out of here.”
He stands to speak to the room. “Close,” he says.
Rogers and Marler stitch Sam’s skin flap back to the side of his face. “That chin of his is going to look awesome,” Marler says. “Not a bad way to start high school,” says Mulliken. He steps away from the table, taking off his gloves, gown and mask. He sits at a table and fills out forms. He glances at a wall clock to note the time.
It is midnight. The surgery has lasted nearly 13 hours.
He files the paperwork and walks out the door and down the empty hallways. Through another set of doors and then into the bowels of the hospital. In the waiting room, he finds Sam’s parents asleep on separate sofas.
He clears his throat. They stir.
David and Debbie Lightner in the recovery area of the Intensive Care Unit, quietly examine the results of the surgery that has just ended. The post-surgical swelling is intense, and it’s hard to see how much progress the surgeons have made.
“Everything is fine,” he tells the Lightners. “All is well.”
“How difficult was it?” David asks.
Mulliken sits on a chair and runs his hands across his face.
“This was very difficult,” Mulliken says. “The most difficult surgery I’ve ever performed. At times we were very discouraged, and it wasn’t easy. But no one ever wanted to give up.”
He yawns. “All is well,” he says, rubbing the back of his neck. “The next step will be fixing the mandible bone, probably next summer. That won’t be a problem.”
The Lightners turn to each other. They hold hands.
“You know, doctor, when I talk with you, I realize how Sam’s face really looked,” David says, his voice breaking. “To me, to us, he’s always been just Sam. I guess we got used to it. To us, he’s just a kid with a big old head.”
Mulliken nods.
“The family doesn’t see it,” he says. “It’s the rest of the world, all of us, the strangers who can’t see beyond the face. That’s the sad part.”
The Lightners stand. They move toward Mulliken but hesitate, not sure of what to do or what to say.
“Thank you,” says Debbie Lightner. She runs her hand across her eyes.
Mulliken smiles. “You’re welcome,” he says.
He turns and disappears through the door.
The Boy Behind the Mask
Tom Hallman Jr.
Photos by Benjamin Brink The Oregonian October 4, 2000, Part 4
“I am Sam, Sam I am”
The doors to Operating Room 16 opened with a bang, and two intensive-care nurses pushed Sam Lightner’s gurney into the hallway, maneuvered it to their left and toward an elevator.
Behind them, a nurse tossed bloody sponges and towels into a bucket on the floor. Another nurse put the final touches on official reports, glancing at the wall clock to note that the boy was leaving the room just after 12:30 a.m. on July 7, 2000. Thirteen hours had passed since a highly specialized team of world-class surgeons had begun Sam’s operation on the morning of July 6.
A thick bandage—brilliant white except for a streak of red left by the blood still oozing through sutures on his neck—encased Sam’s head. An IV line pumped drugs and painkillers into his body. He was heavily sedated, not expected to stir for at least the next 36 hours.
Dr. Jennifer Marler, one of Sam’s three surgeons, pulled off her surgical gown and gloves. In her blue surgical scrubs, she hurried after the bed and pushed her way into the elevator. She wanted be next to Sam when he arrived in the Intensive Care Unit.
The elevator doors opened, and nurses wheeled Sam into a private room. Quickly they plugged lines running from his body into a bank of monitors. They adjusted the screens, and Marler motioned to the nurses. They followed her to the nurse’s station.
She opened Sam’s file and pulled out a color photograph taken in April, when Sam had first been evaluated at Boston’s Children’s Hospital. Sam, Marler explained, was a 14-year-old from Portland, Ore. He’d been born with a venous malformation—a bulging mass of blood vessels and tissue—on the left side of his face. And this, she said, is what he had looked like. She dropped the photograph on the counter. The nurses murmured.
Marler left the file on the counter and walked back into Sam’s room. The frail boy’s body barely filled the bed. His head had swelled to the size of a basketball, completely cloaking his features. Never, Marler told nurses checking on Sam, had she seen a head that big. Make sure it was always supported, she told them. If it somehow dropped off the bed, the weight could cause a spinal injury.
Marler wondered what Sam would look like when the swelling went down in a month. The goal had been to remove the tissue mass, setting the stage for a future surgery on the underlying bone. This first stage of his facial reconstruction might make Sam look 50 percent better, the surgeons figured.
But 50 percent improvement on a facial deformity such as Sam’s— the worst Marler had ever seen—still left a lot of work undone. And Sam was only 10 weeks from his first day at Portland’s Grant High School, a day when he would walk into a mob of judgmental adolescents who’d never seen him before.
Marler remembers standing over the boy’s bed and wondering: Was 50 percent enough?
* * *
When Sam wakes up after surgery, he can communicate only by pressing programmed keys on a small computer suspended in front of his face. He presses Button No. 1 to say, “I hurt.”
On Saturday, July 8, Sam Lightner stirred. His mother, hovering over him, called his name. He briefly opened his eyes before slipping back to sleep. Sam, unable to speak, was supposed to communicate with a small computer. Four responses—“I hurt,” “I need to go to the bathroom,” “yes” and “no”—had been preprogrammed. Sam had only to lift a finger and push one button to answer.
Debbie Lighter asked Sam how he felt.
Sam slowly raised a finger and punched button No. 1.
The pain, nurses told his mother, would be severe for at least three weeks. Even after he left the hospital, he would need painkillers.
That afternoon Marler showed up at the hospital. It was her day off, but she wanted to check on Sam. She recalls reminding herself, as she made her way to the ICU, to look confident, to hide her worry from the Lightners.
The surgery had been the most difficult operation of the lead surgeon’s career and one that had tested the entire team’s resolve. Sam’s anatomy was abnormal, the malformation just a jumble of tissue, blood vessels and nerves. Because X-rays don’t show soft tissue, the nerves lay concealed in the surrounding mass. Damaging a key nerve would have paralyzed the left side of Sam’s face. If that had happened, Sam would have lost the ability to blink his eye, to crinkle his forehead or to smile.
She checked in at the nurse’s station, received an update on Sam and then walked to his room.
She remembers the Lighters standing by the bed, looking at their son. A line from a ventilator—the machine was still breathing for Sam— was hooked into his tracheotomy, the hole in his throat that bypassed the tissue mass. The hole would remain until Sam completed all his surgeries.
Marler made small talk with the Lightners, wondering how she could check on Sam’s nerves. She felt good about the branches leading to his eye and forehead. But what about the branch to his mouth? That area had been hellish in Operating Room 16. She had to know, but Sam seemed to be sound asleep.
She asked if Sam had been awake at all. Yes, said Debbie, he’d woken up enough to stir when she spoke.
Can you make him smile? asked Marler. I need to see if he can smile.
Debbie Lightner leaned over Sam’s bed, moved her head closer to her son’s. Marler inched in right behind. His mother called to Sam.
The only sound in the room was the steady whoosh from the ventilator.
Marler saw the boy’s eyes flutter. Good sign. Try again, she told Debbie.
Sam, Debbie Lighter said, I need you to smile for me.
There was no response, and Debbie Lightner tried again. Sam, she said, smile.
Then, slowly, the outer edge of his mouth began to curl.
And Sam Lightner smiled.
* * *
Before Sam had his surgery he was measured for a mask that would fit over his head and help the left side of his face heat in the best possible position. It’s hot, it itches, and a lump in the fabric hurst. If it’s not cushioned Sam wears it reluctantly, and only when he sleeps.
Eight days after surgery, an internist walked into Sam’s room. The time had come to remove the bandages.
The surgeons who had operated on Sam had told the Lightners to be realistic. The unveiling would be anticlimactic, even disappointing. Sam’s face had taken a beating in the surgery. The buildup of internal fluids would make his face look more distorted than at any time in his life. For the next two months, he would wear an elastic mask each night to force his face into shape and to combat the swelling. The true results, they said, would be revealed in late September or early October.
Even so, Sam could hardly wait to see his new face. Later, he remembered the bandages coming off. The cool air on his face. The doctor backing away from the bed, and his mother moving in to help him.
He was unsteady, a colt learning to walk, and she guided him to the bathroom, to the mirror. The surgeons’ message played in his head— don’t get your hopes up. And then he looked at his reflection.
He focused first on the chin: It was rounder.
Then he examined the entire left side of his face: For the first time in more than a year, he could actually see his left ear, huge and distorted, because the tissue mass that had obscured the ear was gone.
Sam turned to his mother. He smiled, raised his hands to give her a thumbs-up sign. Then she led him back to bed.
Days later, doctors released Sam from the hospital, although they asked that he stay in Boston for several days so that he’d be close to the hospital if an infection set in. Painkillers made the days bearable; so he and his mother explored a museum and visited Fenway Park to see where the Boston Red Sox played.
Then, on July 19, the day before they were to fly home, he felt a lump on his chin.
He showed his mother. When she touched his chin, it hurt. She called the hospital. She was told to bring him right over.
She and Sam walked three blocks from their hotel, checked in and took a seat in the waiting room.
Dr. Jennifer Marler remembers that she was on her way to the laboratory when she spotted the Lightners sitting on a bench. She walked over and asked how they were doing. Debbie explained. Marler asked Sam how he felt. He couldn’t speak. He shrugged his shoulders. He cried.
Marler told them to wait there. She walked over to the receptionist, picked up the telephone, called the lab and canceled her appointment—she had something more important to take care of. She checked with the receptionist, found an empty examination room and collected the Lightners.
Once in the room, she turned the lights low to calm Sam. The mass under his chin, she explained, was not a growth but a buildup of fluid.
He was fine.
What she needed to do, she explained, was to drain the fluid. She administered a local anesthetic, and—while she waited for it to take effect—studied this boy who had dropped into her life 10 months before when a package and a plea for help from Tim Campbell, Sam’s Portland doctor, arrived in her office.
Their relationship had begun with a simple photograph, one Campbell had taken as a way to show the desperation of Sam’s situation. That photo had haunted Marler. It was the photo that led her to repeatedly petition the reluctant team of elite surgeons who would ultimately give in and bring Sam to Boston. It was that photo that would ultimately change his life … and hers.
But on this day in July, she was thinking of a different photo— the picture of a new Sam, a post-surgery Sam, that would join the gallery of photos on her office wall. There his face would appear among the 20 that most touched her during her medical career, the children—some dramatically transformed and some who failed to survive—who had come to her for help. After all she’d been through with this boy, one day Marler wanted to hang a picture of Sam on that wall.
She touched his chin. He did not flinch. She reached for a syringe to drain the fluid from his chin. She wanted to distract him when the needle pierced his skin.
Sam, she remembers saying as she jabbed him, I want you to promise to send me a photograph of you when you get home.
She finished her work, and they all moved to the door, ready to go their separate ways. Marler didn’t know what to say. And then she realized there was nothing to say. She spread her arms wide, pulling Sam close. She hugged him tightly, and tears rolled down her cheeks.
* * *
Debbie Lightner has been trimming Sam’s hair all his life. She spreads newspaper on the kitchen floor, places a chair on the paper and spritzes Sam’s hair with a plastic spray bottle.
The Frontier Airlines jet touched down in Portland on July 20th. Sam Lightner made his way up the aisle and into the crowded terminal. He saw his father, brother and sister carrying balloons reading: “Welcome Home.” They all hugged Sam and told him he looked good.
The surgery was behind in more ways than one. The family’s insurance company, negotiating directly with Children’s Hospital, had reached final resolution on the cost of the surgery. The grand total was $75,000.
It was time to celebrate.
But Sam felt listless. The skin that had been peeled back during surgery, which had been so healthy in Boston, was pale and waxy. His mother remembers feeling his forehead on the flight and thinking he was running a slight fever.
On July 25, the Lightners took Sam to see Dr. Tim Campbell, the pediatric surgeon who had operated on him when he was a day old, the doctor who had sent the plea for help to Jennifer Marler.
Sam shuffled into the waiting room, barely able to pick up his feet. He found the first chair, fell into it and leaned against the wall. He closed his eyes and curled his legs under him. A bead of sweat glistened on his forehead.
The receptionist called his name. With effort, he pushed himself out of the chair and followed her down the hallway to the examination room. His parents trailed behind. He climbed onto the examination table and let his head sag forward. His mother walked over and ran her hands through his brown hair.
The door opened and Campbell, in his light-green surgical scrubs, strolled in carrying Sam’s file.
“Sambo, you old dog,” he said. “How are you?”
Sam slumped against the wall.
“He’s not feeling well,” Debbie Lightner said. ““He had a fever of about 100 this morning. And he seems so tired. I don’t know if it’s from the trip home or what. But he just doesn’t seem himself.”
Campbell put the file down, washed his hands and walked over to the examination table. He leaned close to Sam.
“Sambo,” he said gently, “let me take a look at you.”
Sam raised his face.
“He looks a little swollen,” he said, “but that’s to be expected. Sam, how about lying down for me?” He ran his hands over Sam’s face, checked the file and then walked over and touched Sam’s forehead, feeling the tube the Boston surgeons had sutured under the boy’s scalp. “I think it’s time we take that drain tube out,” he said.
“Now this might hurt a bit, Sam,” Campbell said. “But it’s going to be over quickly.”
Sam tried to sit up, struggling, kicking his legs. “No,” he moaned. “No.”
His father held Sam’s legs. His mother moved to grasp his arms. Even so, he struggled and wiggled. Campbell yanked twice and drew out a clear line. “OK, big boy,” he said. “It’s over.”
Sam sat up, tears streaking his face.
“He’s lost 10 pounds,” Debbie Lightner said. “Some, I know, is from the surgery. But …”
Campbell asked if Sam was eating well, and when he heard that the boy’s appetite had lagged, he sighed.
“I think I’m going to put Sam in the hospital,” he said.
“No,” croaked Sam. “No. Please.”
Campbell patted Sam on the shoulder, kept his hand there and talked to Sam’s parents. “I want him in there for a day or two,” he said. “I want a blood culture, a blood count and I want him on IV antibiotics. I’m sure that blood count will be way off. I think he has an infection. We have too much invested here to take any risk.”
Sam sobbed, appalled that—after all the painful days he’d spent bedridden in Boston—he was headed back to the hospital.
“I know he’s not happy about it,” Campbell said. “I know he wants to go home. But he can get real sick, real fast. Those germs could spread through his body and cut off his windpipe. It could be life-threatening.”
Campbell patted Sam once on the shoulder. “I’m sorry, Sam,” he said. “I really am. Don’t give up, Sam. We’ll lick this.”
“At least we’re home,” David Lightner told his son.
“And it will only be a couple days,” Debbie Lightner added.
An attendant pushed Sam’s wheelchair across an atrium and into the main hospital building. A nurse poked at the boy with a needle while Sam cried and thrashed. She finally connected with a vein and started antibiotics flowing.
Sam checked into a hospital room and spent the next two days watching TV and reading magazines.
The swelling went down. His temperature dropped. And he started slipping out of bed to stroll the hospital halls, dragging his IV setup along with him.
Two days later, as Campbell had promised, Sam checked out of Emanuel and headed for the family home in Northeast Portland. When he got to the house, he looked in the bathroom mirror. With the swelling receding, the left side of his face was noticeably reduced. The bottom of his chin, once distended and pointed, was flat and smooth. Even his left eye, which the mass had pushed and distorted, seemed to be in a more normal position. His parents told him he looked great.
But …
When he scrutinized his face, looking at himself the way he knew strangers would, he realized that he didn’t look dramatically different from before the surgery.
The skin on the left side of his face, even though relieved of the huge mass of tissue that had once supported it, still formed a dome over the deformed bone underneath it. His jaw remained out of alignment, and it still distorted his mouth and teeth. Removing the tissue mass had further exposed his left ear, large, spongy and misshapen.
The surgeons would turn to all those problems the following spring. But in a month, on Aug. 24, 2000, the freshmen will register at Grant High School.
* * *
Even though the first round of his surgery is finished, Sam still has a tracheotomy that requires some special attention during the day. So he and his mother visit the school nurse a week before classes begin at Grant High School to work out the details of his care.
The boy sits on the living-room sofa, lost in his thoughts. His parents are at work. His younger brother and sister are enjoying the last two weeks of summer vacation. He moves through the house, looking at the clock, waiting for his mother to come home and take him to Grant.
Today he will register, officially joining the class of 2004. His sister asks him a question, but he ignores her. He has too many things on his mind.
He walks up to his bedroom, the one with the toy license plate on the door that reads “Sam.”
He hasn’t been back to Grant, Portland’s largest high school, for an official event since the open house on Feb. 3, 2000. That night, he joined more than 1,500 students and parents. He was nervous then.
And now …
He stands and checks out his shirt. Brand-new—pulled from his closet for the first time just for this day. He’s showered, and his hair is neatly combed. He walks downstairs and looks at himself in the mirror. He combs his hair again, carefully pressing the last stubborn strand into place.
He walks into the kitchen to make himself lunch. He opens the refrigerator door—glancing at the list of chores his parents expect him to do each day to earn his $5 weekly allowance. He’s thrown the dirty clothes down the chute to the basement. He’s cleaned the bathroom countertop and swept the floor. He’s picked up the basement and vacuumed the upstairs hallway.
He pulls out a jar of peanut butter and a jar of jam and makes himself a sandwich. His mother walks in the door as he’s finishing it up, and the phone rings. Three of Sam’s Gregory Heights Middle School classmates have gathered at a neighbor’s house and are calling to let him know they’re ready for their ride. Sam’s ready, too. He smoothes his shirt once more and reaches to touch his neck. But when he pulls his hand away, he sees blood on his finger.
Not today.
Not on this day.
Please.
“Mom.”
He points to his neck. Blood oozes from one of his stitches. He dabs at it with a napkin.
“Mom!”
His mother searches for a Band-Aid.
“No one will see this,” his mother says as she gently pushes the strip over the stitch. “Don’t worry.”
The two of them walk out the front door and climb into the family’s old Honda, back down the driveway, turn through tree-lined streets and pull up in front of a wood-frame house. Three strapping young men jump down the steps, move like athletes toward the Lightner car and jump into the back seat. Sam sits next to his mother in front. At 76 pounds, he looks like a little brother along for the ride.
Just as it did on orientation night, traffic clogs the streets around Grant. So Debbie Lightner has to park five blocks away. Sam and his friends step onto the sidewalk and walk through the neighborhood.
On that February evening nearly seven months before, darkness cloaked the long walk, and Sam covered the distance almost invisible to everyone gathering at Grant. Today, the sun shines brightly on streets filled with students.
Sam touches the Band-Aid on his neck. He adjusts his shirt collar, trying to hide it, but nothing works.
He walks on, his pals towering over him. With Grant looming in the distance, all of them grow quiet. The group spreads out as the boys climb the front steps. They head for separate metal doors.
Sam pulls one of the doors open and steps into the front hall. Linoleum floors. Trophy cases. Metal lockers. Noise and laughter and chaos and all the urgency that is about being 14 years old.
Sam’s friends disappear into the crowd, and he stands alone in the midst of the milling mob. An adult hollers instructions, and the students form a rough line that engulfs Sam where he stands. His friends pay no attention to him as they move up and down the line to talk with buddies they have not seen in months.
The line snakes toward the cafeteria, where the students will get their schedules and receive their student identification cards.
Parents show up to pay fees. More students arrive and join the line. The crowd clogs the hall, and someone announces that it will be hours before everyone is registered. Adult volunteers herd the students along, shouting instructions. A teacher brings out a fan to keep everyone cool.
Sam watches new students arrive and walk past him toward the end of the line. He turns to his left, toward a bank of lockers. From this angle, no one can see the left side of his face. Even the students who stand next to him seem unaware of his presence.
“Hey there.”
Sam turns. A Grant administrator motions to him and then walks over.
“How you doing?” he asks as he sticks out his hand.
“Fine,” says Sam, shaking hands while wondering who this man could possibly be.
The man raises his hand, starts to gesture toward Sam’s face, then thinks better of it and lets his hand drop to his side.
“Say, you don’t have to wait here in line,” he says. “I mean …”
The words hang in the air.
“Let me take you down the back way,” he says, rattling a set of keys. “I can get you in and out of here in a couple minutes. Otherwise, you’re going to be here for a couple hours. No reason you should have to wait out here in front of everyone. I know how you must be feeling right now.”
The man steps closer, putting his arm around Sam’s shoulder.
“Let’s go,” he said. “You don’t need this.”
Sam weighs his options and makes a quick response that will be colored, as such things are, by everything that has come before. The years of living with his deformity. The decision to risk a life-threatening surgery. The choices he has made—to take a great chance and to confront life head on. “I am Sam,” read the Dr. Seuss line the nurse posted over his isolette when he was born. “Sam I am.”
He wriggles out from under the man’s arm.
“No,” he says.
“What?”
“I’ll wait with the rest of the students,“ Sam says.
“But you don’t have to.”
“I’ll wait,” Sam says firmly. “This is where I belong.”
* * *
On the first day of school, Sam got to Grant High a few minutes early and navigated to the room listed as his first-period history class. When he arrived, no one else was there and the door was locked—his schedule had the wrong room number.
The line moves, and Sam watches the administrator walk away. There is no turning back. Sam is carried, step by shuffling step, toward the cafeteria. He descends a flight of steps, walks through a set of double metal doors and pauses, looking out at a sea of students.
Then the line carries him forward to the first of several registration stations along the cafeteria’s wall. Brian Doran, Sam’s friend from Gregory Heights, spots him in line, hurries over and hands him a green piece of paper with a locker number and combination on it. Brian, who arrived earlier, has already claimed the locker and requested Sam as a partner.
Sam feels someone touch his shoulder and turns to face Molly Paterno, an old friend from his neighborhood.
“I was thinking about you all summer, Sam,” she says. “I wondered if you had the surgery.”
She studies him.
“Oh, Sam,” she says. “You look great.”
Sam moves more easily as the line works its way from station to station. He studies his schedule.
“Sam?”
Emilie Bushlen bustles up and leans close.
“Sam, can I see your schedule?”
He hands her his slip of paper.
“Sam,” she squeals. “We got word-processing together.”
He blushes.
The line moves forward. The next stop is for yearbook pictures. Sam looks at the order form, trying to figure out what picture package to order. He selects Package E, the one that will give him two extra prints. One will go to Dr. John Mulliken, the lead surgeon in Boston.
The other has a place waiting for it on Dr. Jennifer Marler’s wall.
He hands the form to the photographer, who tells him where to sit and how to pose. “OK, kiddo,” the photographer says. “Here we go.”
He lifts the camera.
Sam Lightner looks straight ahead. This is for the yearbook. This is for history.
He smiles. Broadly.
And a brilliant flash illuminates his face. (The End)
教育家们对弗莱施大发雷霆。他让他们显得愚蠢无能。他们知道自己并不愚蠢。他们完成了历史上最大的反智阴谋。虽然杜威、桑代克和卡特尔已经去世,但他们的弟子,哥伦比亚大学的阿瑟-盖茨(Arthur I. Gates)和芝加哥大学的威廉-斯科特-格雷(William Scott Gray)决心继承导师的事业。1955 年,阅读教授们组织了国际阅读协会,以维护 “看-说 “在小学阅读教学中的主导地位。如今,”看图说话 “以各种面目渗透到教育市场的各个角落,而且被广泛地、不加批判地接受,以至于教师或家长需要具备专业知识,才能分辨其中的好坏和利弊。
Samuel L. Blumenfeldis the author of six books on education: How to Start Your Own School and Why You Need One (1972), The New Illiterates (1973), How to Tutor (1973), Is Public Education Necessary? (1981), Alpha-Phonics: A Primer for Beginning Readers (1983), and NEA: Trojan Horse in American Education (1984). His writings have appeared frequently in major journals as well. He has taught in both public and private schools, including a private school for children with learning and behavioral problems.
In a bizarre trend sweeping social media, men claim that they think about the Roman Empire as often as once a week — leaving women baffled.
The trend seemingly originated early this month after one user posted to X — previously known as Twitter — sharing her husband’s response after asking him: “How often do you think about the Roman Empire?”.
To that, her husband responded without missing a beat: “Every day”.
After the Tweet started to gain traction across X, other women decided to test the theory, which prompted many videos on TikTok showing them asking their male partners the same question.
And, weirdly enough, the theory was quickly proven, as many men in the videos confidently announced they think about the days of Marcus Aurelius frequently, sometimes as much as once a week.
It’s clear the newly encountered phenomenon had many totally baffled as to how many male brains do, in fact, lead to Rome, with the TikTok hashtag #romanempire now reaching over 900 million views.
“I’m convinced they’re all just pulling a prank on us,” one user wrote.
“Mine said every time it rains,” another added.
One shocked commenter said: “This trend is rocking my whole world”.
“My husband said “it is a duty of a man to think about the Roman Empire” like wtf?” another user added.
But the jokes haven’t come without the queries, with many eager to get to the bottom of the Roman Empire thought process, figuring out why a government formed 2000 years ago consumes so many men’s hearts and minds.
Hannah Cornwell, a historian of the ancient world at Britain’s Birmingham University, theorized it could be because of the images conjured when Ancient Rome is mentioned — which is further imprinted by Hollywood blockbusters like Gladiator and Spartacus.
Cornwell told the Washington Post that “an image of the Roman legion, the imperial eagle and that sort of military aspect” are the first things that come to mind when thinking of the Roman Empire.
Delving into the psychology aspect a bit further, Dr Alicia Brown from Turning Tides Psychology suggests that another reason could be its association with “strength”.
According to Brown, historically and culturally, men are often aligned with ideals of power, and the Roman Empire epitomizes tales of strength, conquest, and grandeur.
Historical tales from that era evoke intrigue, particularly for those interested in understanding the origins of societal strength and resilience.
Despite it seeming like a gendered-influenced thought pattern, women have come out of the woodwork to counteract it, stating that thinking about the Roman Empire has more to do with personal fascination rather than having a “male brain”.
“Yes, straight men do spend an indescribable amount of time thinking about the Roman Empire — but so does everyone else who’s curious about the past and the lessons it offers about modern culture,” said Cecily Mauran on Mashable.




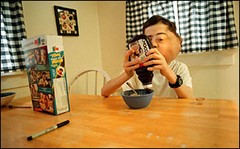
 The computer room in Sam’s house is out of main traffic patterns, and it’s a place where Sam can slip off into his own world. On the Internet, Sam is just another screen name in a chat room, where his words speak for themselves, unfiltered by his distorted voice or his appearance.
The computer room in Sam’s house is out of main traffic patterns, and it’s a place where Sam can slip off into his own world. On the Internet, Sam is just another screen name in a chat room, where his words speak for themselves, unfiltered by his distorted voice or his appearance.